

Validation of the Graded Prognostic Assessment for Melanoma Using Molecular Markers (Melanoma-molGPA)
- PMID: 29416574
- PMCID: PMC5798262
- DOI: 10.14740/jocmr3248w
Validation of the Graded Prognostic Assessment for Melanoma Using Molecular Markers (Melanoma-molGPA)
Abstract
Background: It has been suggested to replace the diagnosis-specific graded prognostic assessment (DS-GPA, based on performance status and number of brain metastases) for patients with primary malignant melanoma with the new Melanoma-molGPA. The latter is a more complex assessment, which also includes BRAF mutation status, age and extracranial metastases. To test the performance of the Melanoma-molGPA, we performed a validation study of this new survival prediction tool.
Methods: A retrospective analysis of patients treated at two different academic institutions was performed. The four-tiered Melanoma-molGPA was calculated as suggested in the original study.
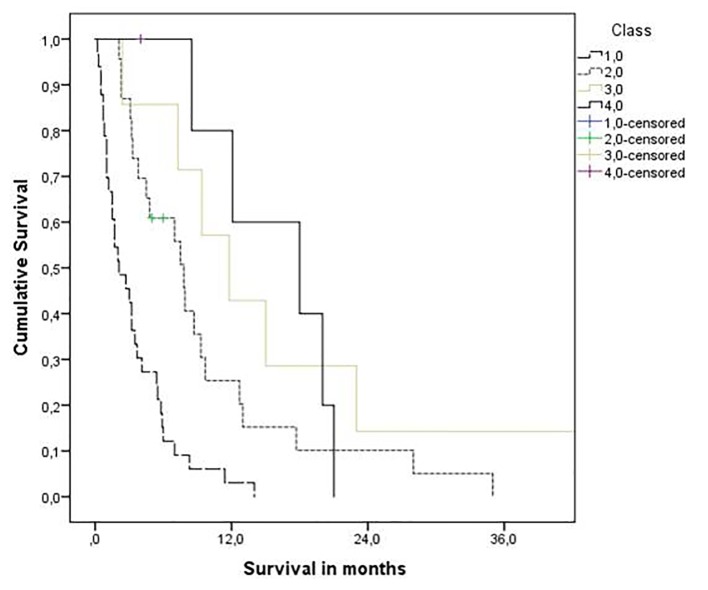
Results: Median overall survival was 5.4 months (95% confidence interval: 3.1 - 7.7 months). Median survival in the four prognostic classes was 2.1, 7.8, 11.8, and 18.0 months, respectively. The 1-year survival rates were 3%, 25%, 43%, and 80%, respectively. The difference between the Kaplan-Meier curves was significant (P = 0.0001, log-rank test).
Conclusions: The present survival outcomes support the use of the Melanoma-molGPA. However, survival was better in each of the four groups in the original study. Possible reasons include lead-time bias and different treatment policies.
Keywords: Brain metastases; Melanoma; Prognostic score; Radiosurgery; Radiotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gaudy-Marqueste C, Dussouil AS, Carron R, Troin L, Malissen N, Loundou A, Monestier S. et al. Survival of melanoma patients treated with targeted therapy and immunotherapy after systematic upfront control of brain metastases by radiosurgery. Eur J Cancer. 2017;84:44–54. doi: 10.1016/j.ejca.2017.07.017. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials