

Vasospasm in the setting of traumatic bilateral carotid-cavernous fistulas and its effect on treatment
- PMID: 29416904
- PMCID: PMC5791513
- DOI: 10.4103/sni.sni_190_17
Vasospasm in the setting of traumatic bilateral carotid-cavernous fistulas and its effect on treatment
Abstract
Background: Direct, Type A, cavernous-carotid fistulas (CCFs) are predominantly caused by head trauma, especially when basilar skull fractures are present. Transarterial endovascular treatment of direct CCFs is the preferred method of treatment. Bilateral CCFs are estimated to be present in 1-2% of the cases. The treatment of bilateral CCFs is difficult often requiring a combination of endovascular and open surgical approaches.
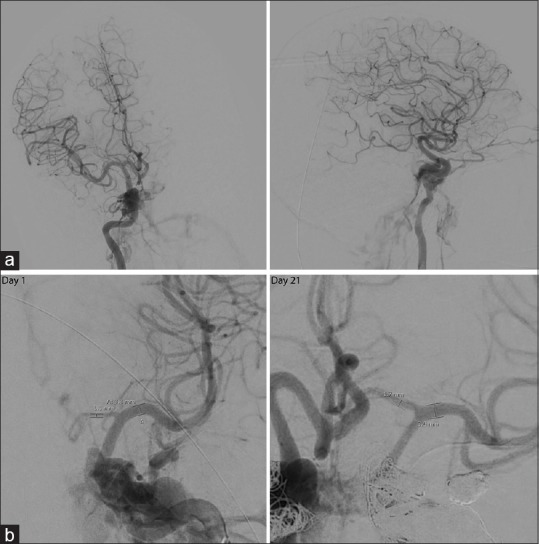
Case description: We present a case of traumatic bilateral CCFs presenting with vasospasm of the anterior circulation seen on the initial angiogram on day 1 and our treatment paradigm.
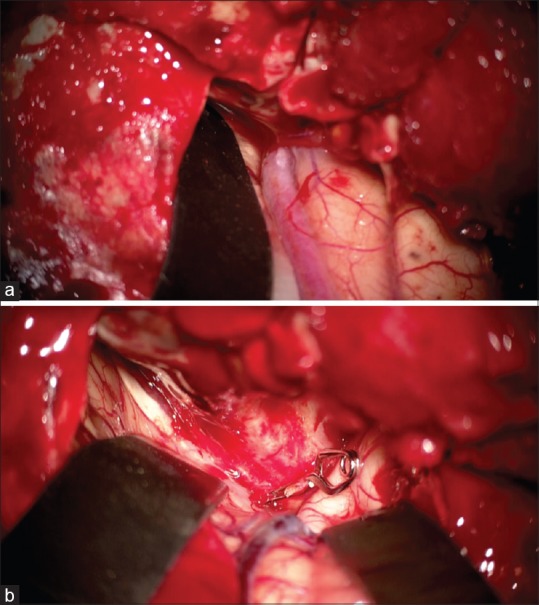
Conclusion: This case illustrates the challenges in managing bilateral CCFs as well as the changes in collateral circulation because of cerebral vasospasm which affected our treatment paradigm.
Keywords: Caroticocavernous fistula; carotid cavernous fistula; cerebral vasospasm; head trauma; traumatic subarachnoid hemorrhage.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
Spontaneous resolution of direct carotid-cavernous fistulas: case series and literature review.Interv Neuroradiol. 2019 Feb;25(1):71-89. doi: 10.1177/1591019918800220. Epub 2018 Sep 23. Interv Neuroradiol. 2019. PMID: 30244626 Free PMC article. Review.
-
Carotid cavernous fistula (CCF) treatment approaches: A systematic literature review and meta-analysis of transarterial and transvenous embolization for direct and indirect CCFs.Clin Neurol Neurosurg. 2021 May;204:106601. doi: 10.1016/j.clineuro.2021.106601. Epub 2021 Mar 20. Clin Neurol Neurosurg. 2021. PMID: 33774507
-
Brainstem compression caused by bilateral traumatic carotid cavernous fistulas: case report.Neurosurgery. 2010 Oct;67(4):E1160-3; discussion E1163-4. doi: 10.1227/NEU.0b013e3181edb148. Neurosurgery. 2010. PMID: 20881535
-
Multimodal Management of Carotid-Cavernous Fistulas.World Neurosurg. 2020 Jan;133:e796-e803. doi: 10.1016/j.wneu.2019.10.004. Epub 2019 Oct 9. World Neurosurg. 2020. PMID: 31605852
-
Endovascular Modalities for the Treatment of Cavernous Sinus Arteriovenous Fistulas: A Single-Center Experience.J Stroke Cerebrovasc Dis. 2015 Dec;24(12):2824-38. doi: 10.1016/j.jstrokecerebrovasdis.2015.08.016. Epub 2015 Sep 26. J Stroke Cerebrovasc Dis. 2015. PMID: 26409721
References
-
- Armonda RA, Bell RS, Vo AH, Ling G, DeGraba TJ, Crandall B, et al. Wartime traumatic cerebral vasospasm: Recent review of combat casualties. Neurosurgery. 2006;59:1215–25. discussion 1225. - PubMed
-
- Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62:248–56. - PubMed
-
- Bavinzski G, Killer M, Gruber A, Richling B. Treatment of post-traumatic carotico-cavernous fistulae using electrolytically detachable coils: Technical aspects and preliminary experience. Neuroradiology. 1997;39:81–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources