

Maturation of tertiary lymphoid structures and recurrence of stage II and III colorectal cancer
- PMID: 29416939
- PMCID: PMC5798199
- DOI: 10.1080/2162402X.2017.1378844
Maturation of tertiary lymphoid structures and recurrence of stage II and III colorectal cancer
Abstract
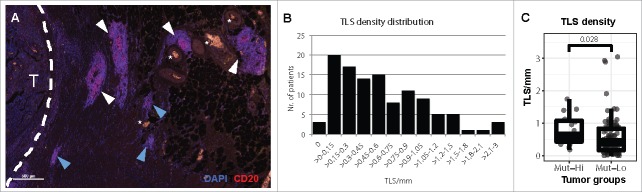
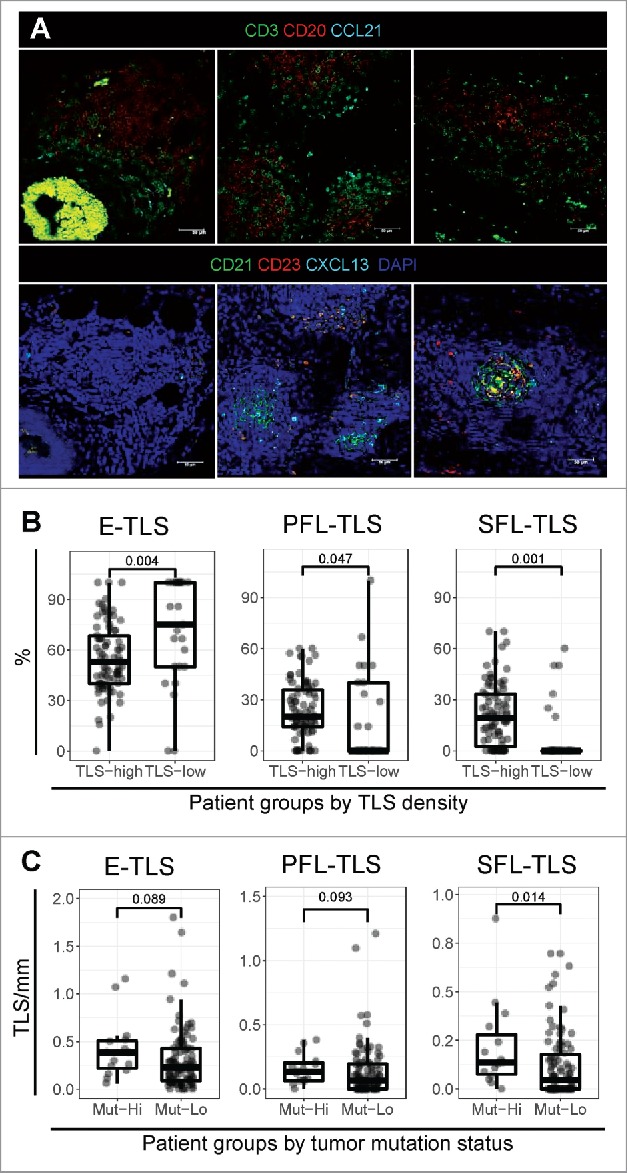
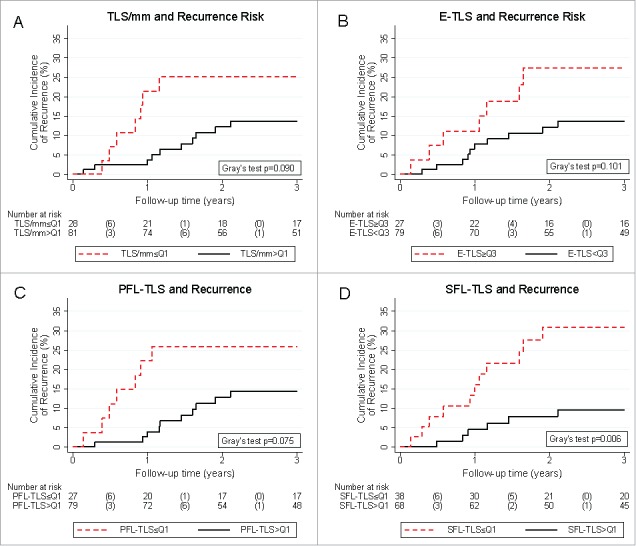
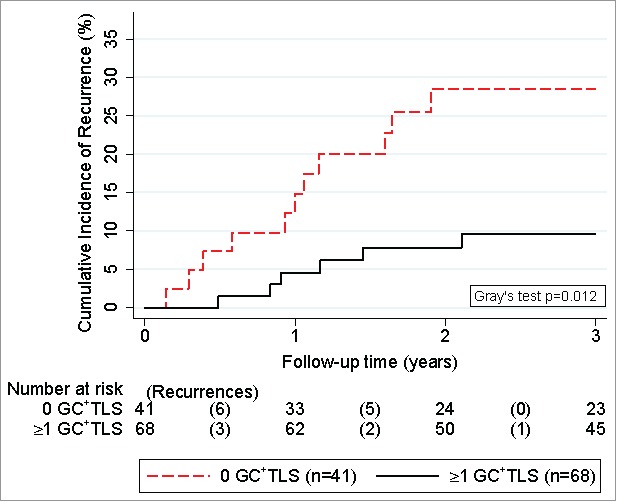
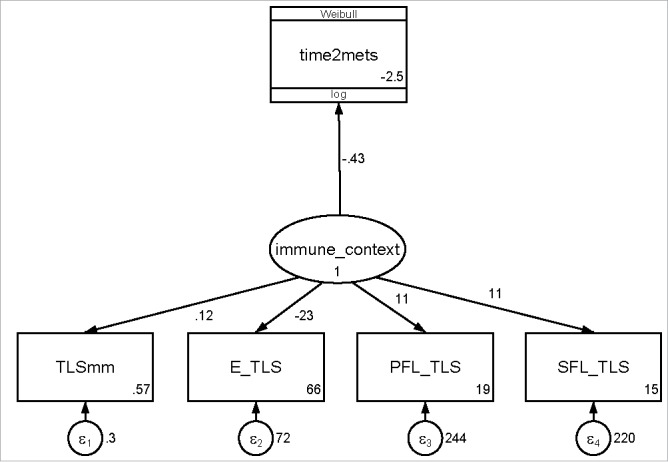
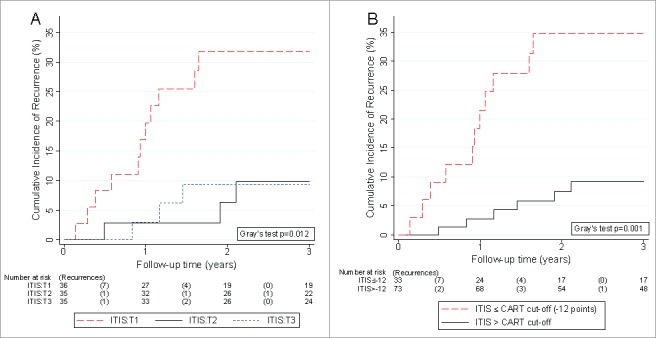
Tertiary lymphoid structures (TLS) are associated with favorable outcome in non-metastatic colorectal carcinoma (nmCRC), but the dynamics of TLS maturation and its association with effective anti-tumor immune surveillance in nmCRC are unclear. Here, we hypothesized that not only the number of TLS but also their composition harbors information on recurrence risk in nmCRC. In a comprehensive molecular, tissue, laboratory, and clinical analysis of 109 patients with stage II/III nmCRC, we assessed TLS numbers and degree of maturation in surgical specimens by multi-parameter immunofluorescence of follicular dendritic cell (FDC) and germinal center (GC) markers. TLS formed in most tumors and were significantly more prevalent in highly-microsatellite-instable (MSI-H) and/or BRAF-mutant nmCRC. We could distinguish three sequential TLS maturation stages which were characterized by increasing prevalence of FDCs and mature B-cells: [1] Early TLS, composed of dense lymphocytic aggregates without FDCs, [2] Primary follicle-like TLS, having FDCs but no GC reaction, and [3] Secondary follicle-like TLS, having an active GC reaction. A simple integrated TLS immunoscore reflecting these parameters identified a large subgroup of nmCRC patients with a very low risk of recurrence independently of clinical co-variables such as ECOG performance status, age, stage, and adjuvant chemotherapy. We conclude that (1) mismatch repair and BRAF mutation status are associated with the formation of TLS in nmCRC, (2) TLS formation in nmCRC follows sequential maturation steps, culminating in germinal center formation, and (3) this maturation process harbors important prognostic information on the risk of disease recurrence.
Keywords: Crohn's-like reaction; colorectal cancer; germinal center; immunoscore; recurrence; risk factor; structural equation model; tertiary lymphoid structures.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous