

Advanced Imaging Techniques in Skull Base Osteomyelitis Due to Malignant Otitis Externa
- PMID: 29416952
- PMCID: PMC5778178
- DOI: 10.1007/s40134-018-0263-y
Advanced Imaging Techniques in Skull Base Osteomyelitis Due to Malignant Otitis Externa
Abstract
Purpose of review: To give an up-to-date overview of the strengths and weaknesses of current imaging modalities in diagnosis and follow-up of skull base osteomyelitis (SBO).
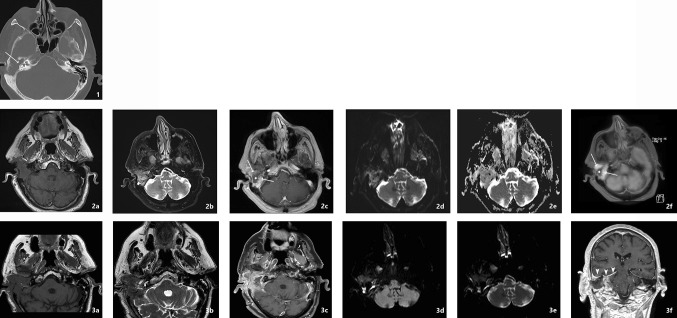
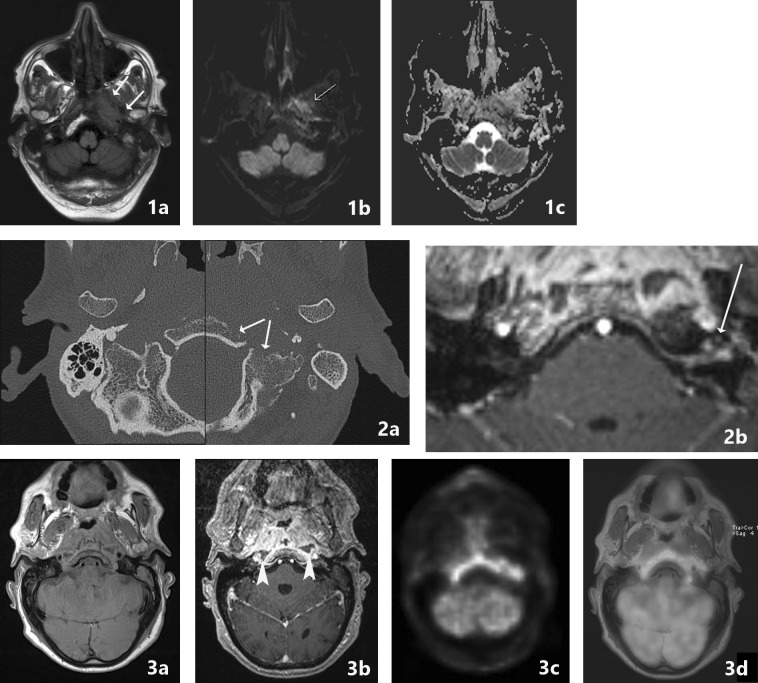
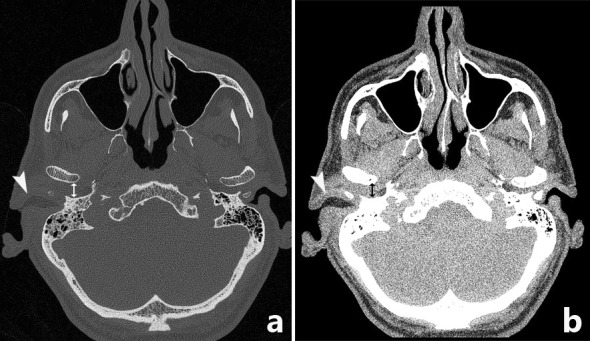
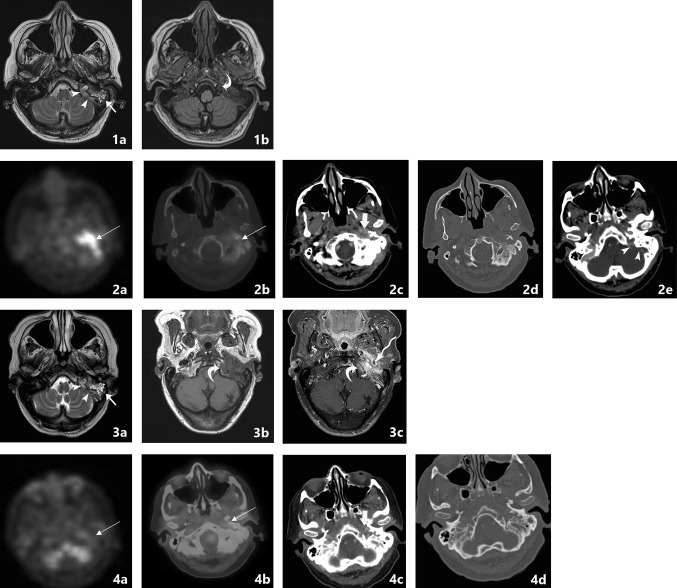
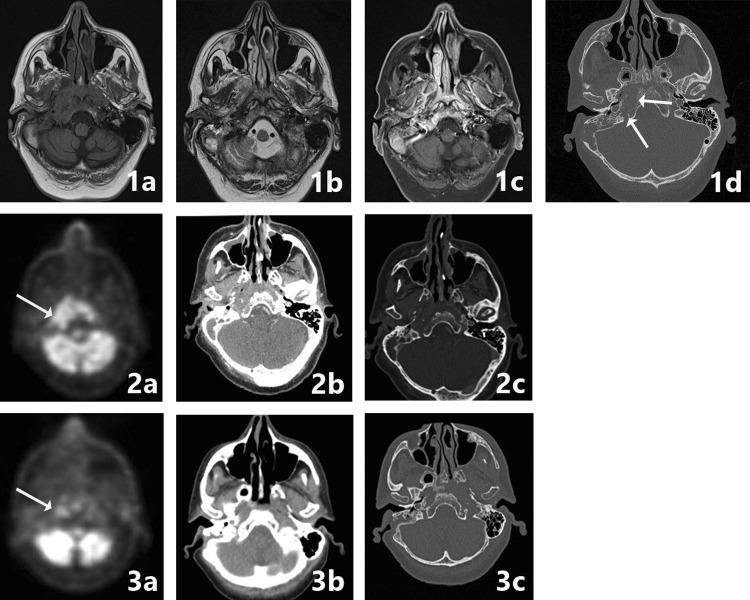
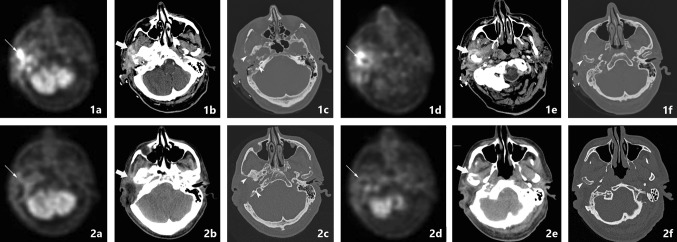
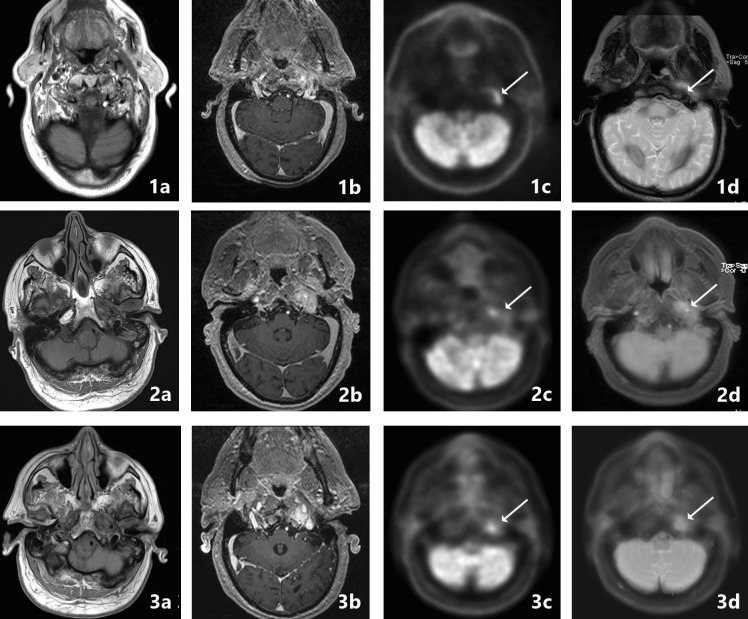
Recent findings: CT and MRI are both used for anatomical imaging, and nuclear techniques aid in functional process imaging. Hybrid techniques PET-CT and PET-MRI are the newest modalities which combine imaging strengths.
Summary: No single modality is able to address the scope of SBO. A combination of functional and anatomical imaging is needed, in the case of newly suspected SBO we suggest the use of PET-MRI (T1, T2, T1-FS-GADO, DWI) and separate HRCT for diagnosis and follow-up.
Keywords: CT; MRI; Malignant otitis externa; PET-CT; PET-MRI; Skull base osteomyelitis.
Conflict of interest statement
Compliance with Ethical GuidelinesA.M.J.L. van Kroonenburgh, W.L. van der Meer, R.J.P. Bothof, Mark van Tilburg, and Joost van Tongeren each declare no potential conflicts of interest. A.A. Postma reports speakers’ fees from Bayer and Siemens Healthcare. Dr. Postma is a section editor for Current Radiology Reports.This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures

References
-
- • Adams A, Offiah C. Central skull base osteomyelitis as a complication of necrotizing otitis externa: imaging findings, complications, and challenges of diagnosis. Clin Radiol. 2012;67(10):e7–e16. A well written article with CT, MRI and PET-CT examples of SBO. - PubMed
-
- •• Grandis JR, Branstetter BFT, Yu VL. The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations. Lancet Infect Dis. 2004;4(1):34–9. A detailed and well illustrated article of SBO spreading patterns with multiple examples. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials