

Anatomic distribution of hematoma following pelvic fracture
- PMID: 29419325
- PMCID: PMC6190786
- DOI: 10.1259/bjr.20170840
Anatomic distribution of hematoma following pelvic fracture
Abstract
Objective: To assess the extent of pelvic hemorrhage on CT and to estimate its significance on outcome in patients with blunt high-energy pelvic trauma.
Methods: 576 patients with blunt high-energy pelvic fractures in 2005-2011 were identified in the hospital's Trauma Registry (a major Trauma Center). 60 of these met our further inclusion criteria of initial systolic blood pressure ≤100 mmHg and pelvic-related hemorrhage. CT scans of the patients were reviewed with regard to pelvic and abdominal retroperitoneal hemorrhage, type of fracture (Tile classification) and associated injuries. Extent of hemorrhage was correlated to 30-day mortality, transfusion requirements and need of angiography. Statistical methods include Pearson's Χ2 test and Fisher's exact test.
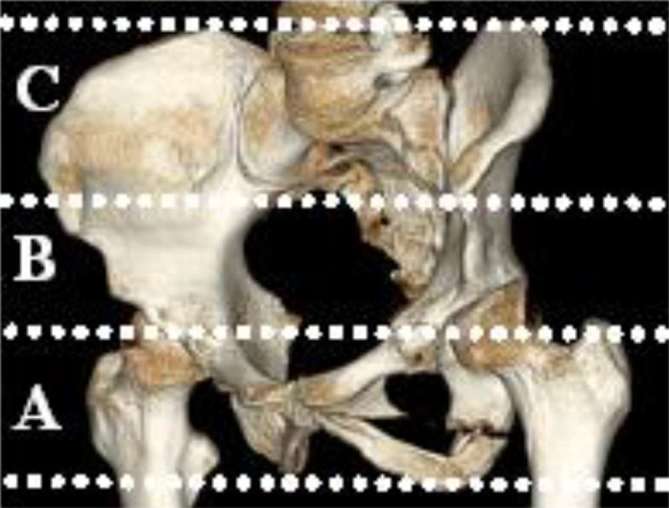
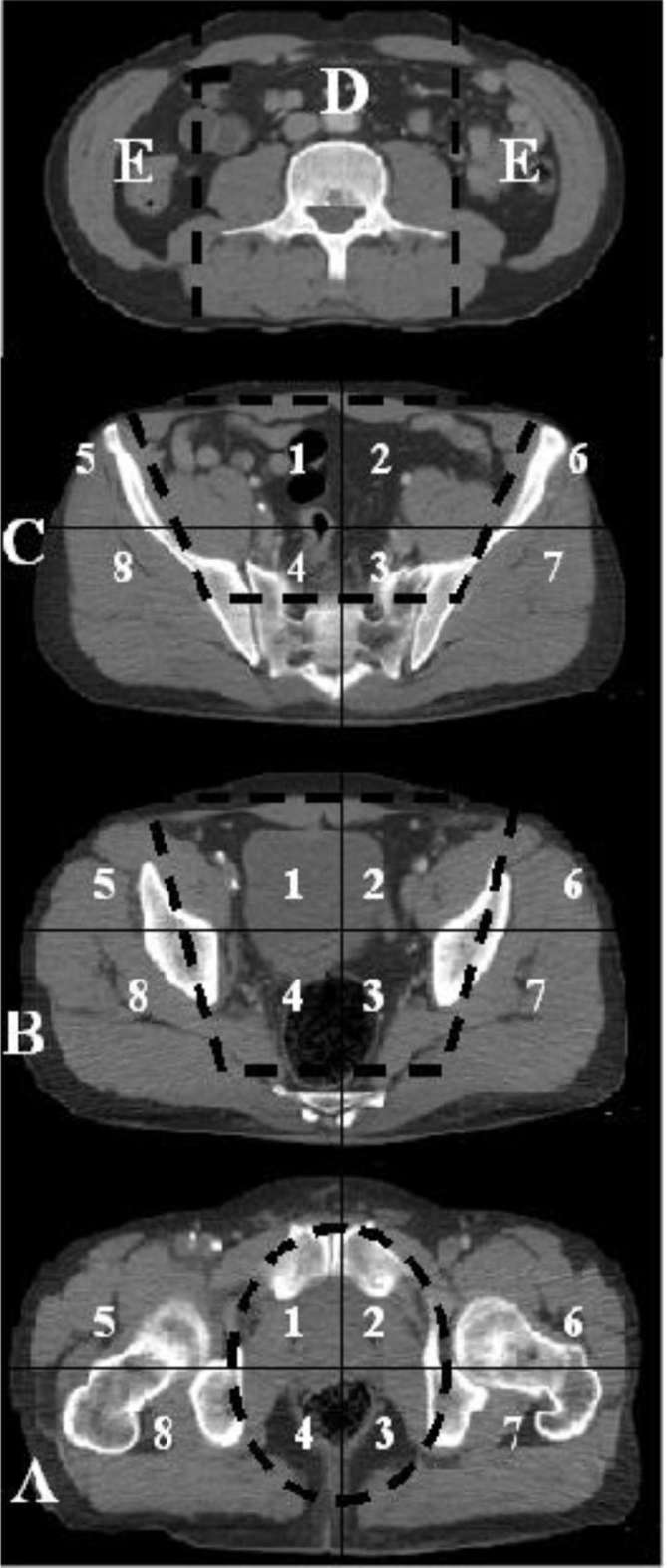
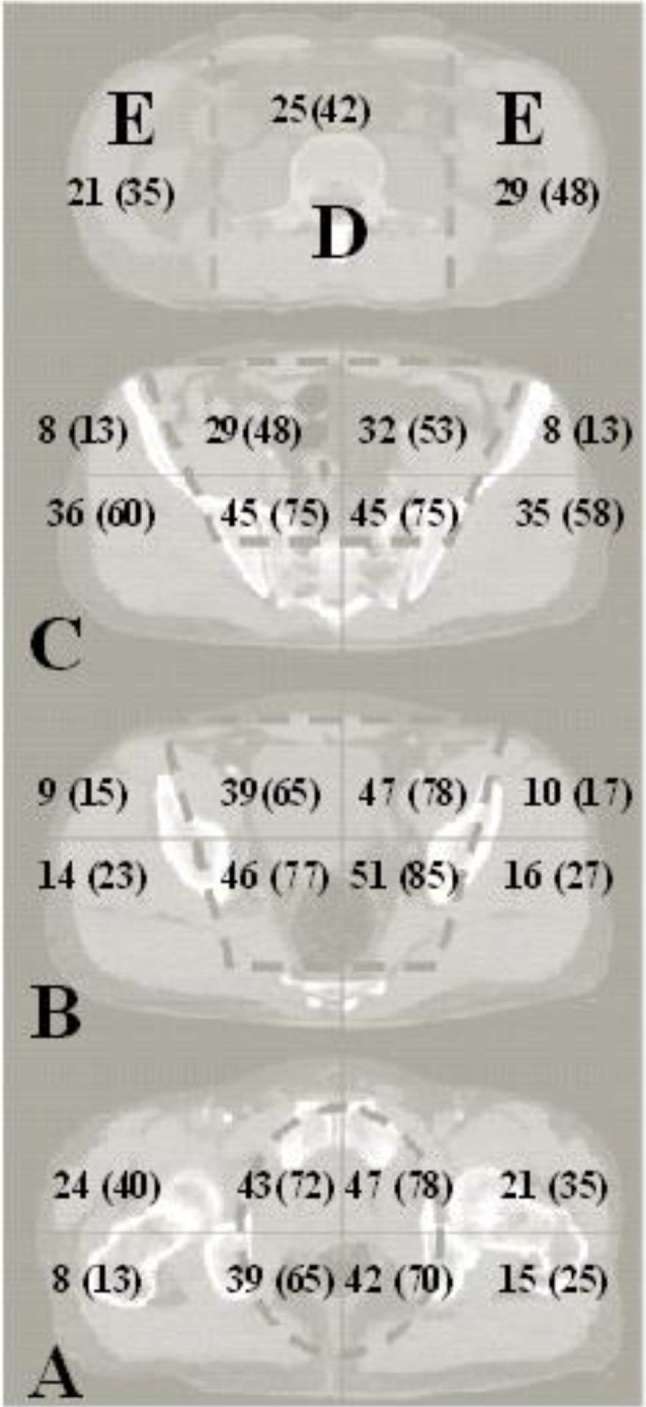
Results: Pelvic hemorrhage extended beyond the pelvis to the abdominal area in 47% of the patients, to the thighs in 25% and to the gluteal areas in 81%. The extent of hemorrhage was significantly associated with the need for blood transfusions (p = 0.011) and angiography (p < 0.001), but not with 30-day mortality.
Conclusion: Traumatic pelvic bleeding frequently extends beyond the true pelvis. Extrapelvic hemorrhage correlates with an increased need of transfusions, but not with 30-day mortality. Further studies are needed to assess whether present techniques to control pelvic bleeding need to be modified in order to further reduce mortality in traumatic pelvic hemorrhage. Advances in knowledge: The study shows localization of pelvic hemorrhage in trauma patients. It may help to select patients in need of further interventions to control bleeding.
Figures
References
-
- Krieg JC, Mohr M, Ellis TJ, Simpson TS, Madey SM, Bottlang M. Emergent stabilization of pelvic ring injuries by controlled circumferential compression: a clinical trial. J Trauma 2005; 59: 659–64. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
