

Neighborhood Socioeconomic Status and Outcomes Following the Norwood Procedure: An Analysis of the Pediatric Heart Network Single Ventricle Reconstruction Trial Public Data Set
- PMID: 29420218
- PMCID: PMC5850235
- DOI: 10.1161/JAHA.117.007065
Neighborhood Socioeconomic Status and Outcomes Following the Norwood Procedure: An Analysis of the Pediatric Heart Network Single Ventricle Reconstruction Trial Public Data Set
Abstract
Background: Children with single ventricle heart disease require frequent interventions and follow-up. Low socioeconomic status (SES) may limit access to high-quality care and place these children at risk for poor long-term outcomes.
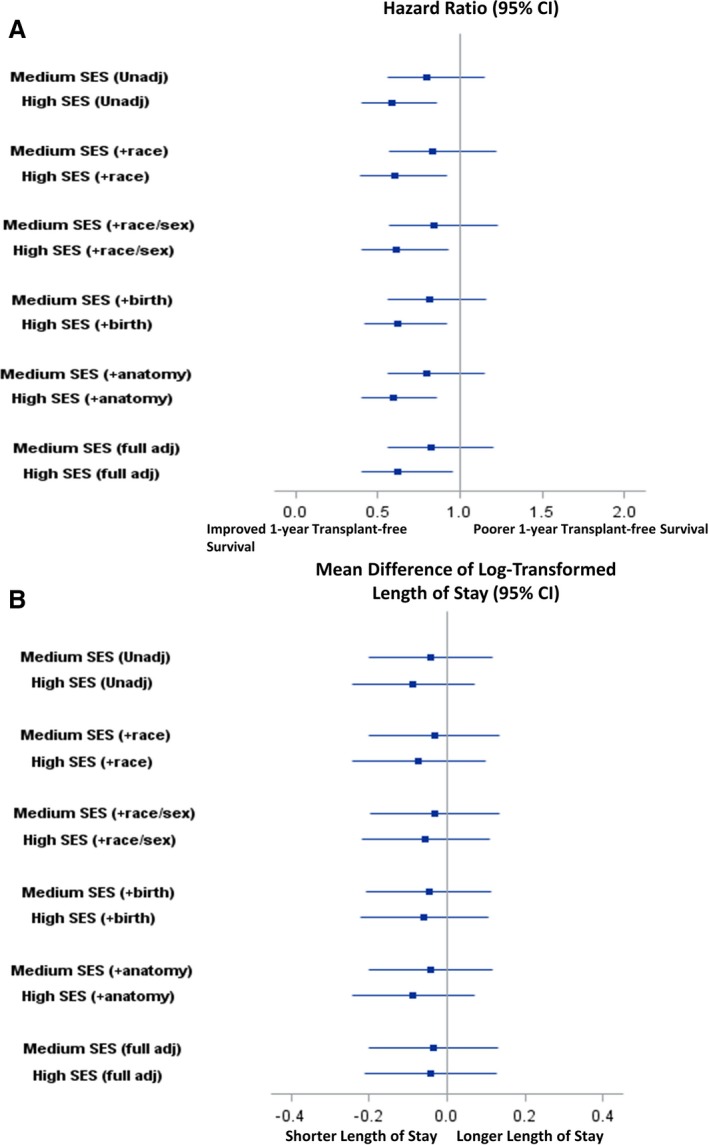
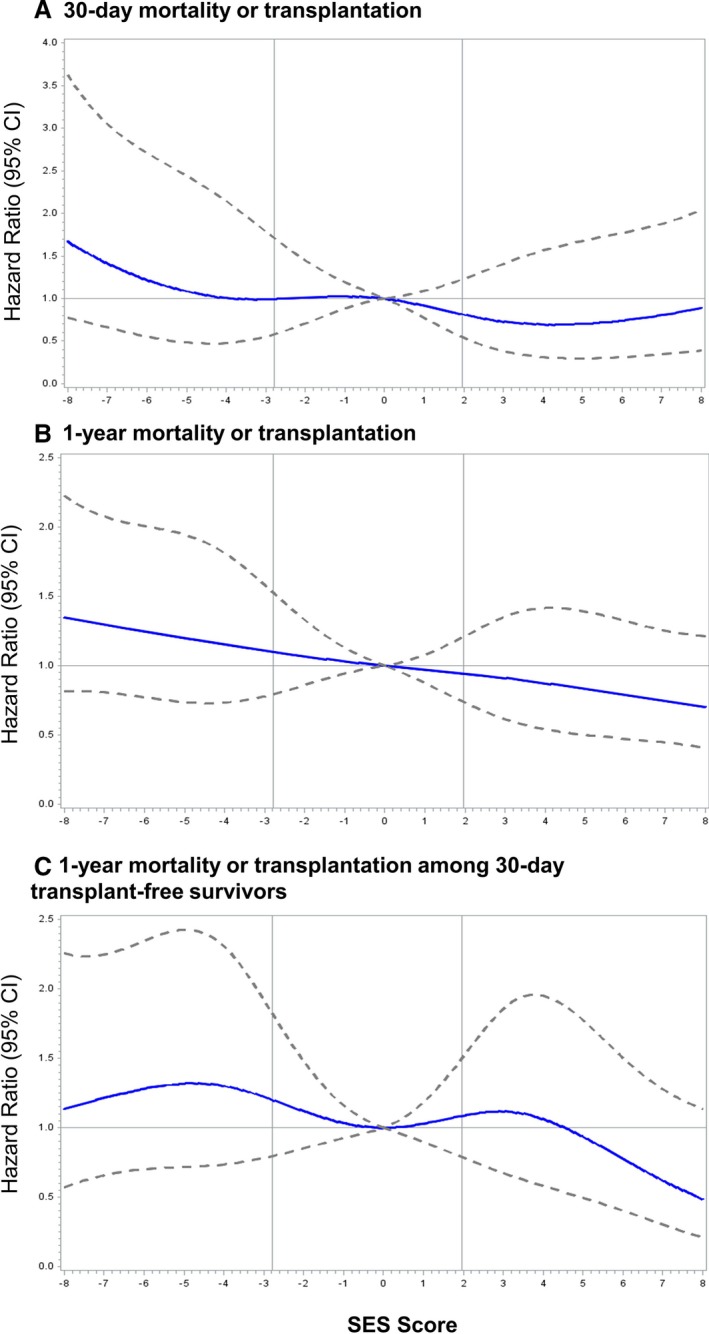
Methods and results: Data from the SVR (Pediatric Heart Network Single Ventricle Reconstruction Trial Public Use) data set were used to examine the relationship of US neighborhood SES with 30-day and 1-year mortality or cardiac transplantation and length of stay among neonates undergoing the Norwood procedure (n=525). Crude rates of death or transplantation at 1 year after Norwood were highest for patients living in neighborhoods with low SES (lowest tertile 37.0% versus middle tertile 31.0% versus highest tertile 23.6%, P=0.024). After adjustment for patient demographics, birth characteristics, and anatomy, patients in the highest SES tertile had significantly lower risk of death or transplant than patients in the lowest SES tertile (hazard ratio 0.62, 95% confidence interval, 0.40, 0.96). When SES was examined continuously, the hazard of 1-year death or transplant decreased steadily with increasing neighborhood SES. Hazard ratios for 30-day transplant-free survival and 1-year transplant-free survival were similar in magnitude. There were no significant differences in length of stay following the Norwood procedure by SES.
Conclusions: Low neighborhood SES is associated with worse 1-year transplant-free survival after the Norwood procedure, suggesting that socioeconomic and environmental factors may be important determinants of outcome in critical congenital heart disease. Future studies should investigate aspects of SES and environment amenable to intervention.
Clinical trial registration: URL:http://www.clinicaltrials.gov> http://www.clinicaltrials.gov. Unique identifier: NCT00115934.
Keywords: single ventricle; socioeconomic position; surgery; survival.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures


Similar articles
-
Risk factors for hospital morbidity and mortality after the Norwood procedure: A report from the Pediatric Heart Network Single Ventricle Reconstruction trial.J Thorac Cardiovasc Surg. 2012 Oct;144(4):882-95. doi: 10.1016/j.jtcvs.2012.05.019. Epub 2012 Jun 15. J Thorac Cardiovasc Surg. 2012. PMID: 22704284 Free PMC article. Clinical Trial.
-
Comparison of right ventricle-pulmonary artery shunt position in the Single Ventricle Reconstruction trial.J Thorac Cardiovasc Surg. 2017 Jun;153(6):1490-1500.e1. doi: 10.1016/j.jtcvs.2016.10.104. Epub 2017 Feb 9. J Thorac Cardiovasc Surg. 2017. PMID: 28274556
-
Transplantation-free survival and interventions at 3 years in the single ventricle reconstruction trial.Circulation. 2014 May 20;129(20):2013-20. doi: 10.1161/CIRCULATIONAHA.113.006191. Epub 2014 Apr 4. Circulation. 2014. PMID: 24705119 Free PMC article. Clinical Trial.
-
The Norwood procedure: in favor of the RV-PA conduit.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2013;16(1):52-8. doi: 10.1053/j.pcsu.2013.01.002. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2013. PMID: 23561818 Review.
-
Long-term progression and survival following Norwood Single Ventricle Reconstruction.Curr Opin Cardiol. 2015 Jan;30(1):95-9. doi: 10.1097/HCO.0000000000000129. Curr Opin Cardiol. 2015. PMID: 25389656 Review.
Cited by
-
Socioeconomic Influences on Outcomes Following Congenital Heart Disease Surgery.Pediatr Cardiol. 2024 Jun;45(5):1072-1078. doi: 10.1007/s00246-024-03451-7. Epub 2024 Mar 12. Pediatr Cardiol. 2024. PMID: 38472658 Free PMC article.
-
Weight impacts 1-year congenital heart surgery outcomes independent of race/ethnicity and payer.Cardiol Young. 2021 Feb;31(2):279-285. doi: 10.1017/S1047951120003911. Epub 2020 Nov 19. Cardiol Young. 2021. PMID: 33208210 Free PMC article.
-
An Examination of Social Determinants of Health and their Association with Preventable and Urgent Readmissions in Pediatric Acute Care Cardiology.Pediatr Cardiol. 2025 Apr 30. doi: 10.1007/s00246-025-03879-5. Online ahead of print. Pediatr Cardiol. 2025. PMID: 40301165
-
Racial and Educational Isolation are Associated with Worse Outcomes in Congenital Heart Disease.Pediatr Cardiol. 2025 Jan 15:10.1007/s00246-025-03772-1. doi: 10.1007/s00246-025-03772-1. Online ahead of print. Pediatr Cardiol. 2025. PMID: 39815062
-
Racial and Ethnic Variation in ECMO Utilization and Outcomes in Pediatric Cardiac ICU Patients.JACC Adv. 2023 Oct 6;2(9):100634. doi: 10.1016/j.jacadv.2023.100634. eCollection 2023 Nov. JACC Adv. 2023. PMID: 38938717 Free PMC article.
References
-
- Jacobs JP, Mayer JE Jr, Mavroudis C, O'Brien SM, Austin EH III, Pasquali SK, Hill KD, Overman DM, St Louis JD, Karamlou T, Pizarro C, Hirsch‐Romano JC, McDonald D, Han JM, Becker S, Tchervenkov CI, Lacour‐Gayet F, Backer CL, Fraser CD, Tweddell JS, Elliott MJ, Walters H III, Jonas RA, Prager RL, Shahian DM, Jacobs ML. The Society of Thoracic Surgeons Congenital Heart Surgery Database: 2017 update on outcomes and quality. Ann Thorac Surg. 2017;103:699–709. - PubMed
-
- Alsoufi B, Mori M, Gillespie S, Schlosser B, Slesnick T, Kogon B, Kim D, Sachdeva R, Kanter K. Impact of patient characteristics and anatomy on results of Norwood operation for hypoplastic left heart syndrome. Ann Thorac Surg. 2015;100:591–598. - PubMed
-
- Tweddell JS, Sleeper LA, Ohye RG, Williams IA, Mahony L, Pizarro C, Pemberton VL, Frommelt PC, Bradley SM, Cnota JF, Hirsch J, Kirshbom PM, Li JS, Pike N, Puchalski M, Ravishankar C, Jacobs JP, Laussen PC, McCrindle BW; Pediatric Heart Network Investigators . Intermediate‐term mortality and cardiac transplantation in infants with single‐ventricle lesions: risk factors and their interaction with shunt type. J Thorac Cardiovasc Surg. 2012;144:152–159. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
