

Flexible endoscopy for pediatric tracheobronchial metallic stent placement, maintenance and long-term outcomes
- PMID: 29420596
- PMCID: PMC5805307
- DOI: 10.1371/journal.pone.0192557
Flexible endoscopy for pediatric tracheobronchial metallic stent placement, maintenance and long-term outcomes
Abstract
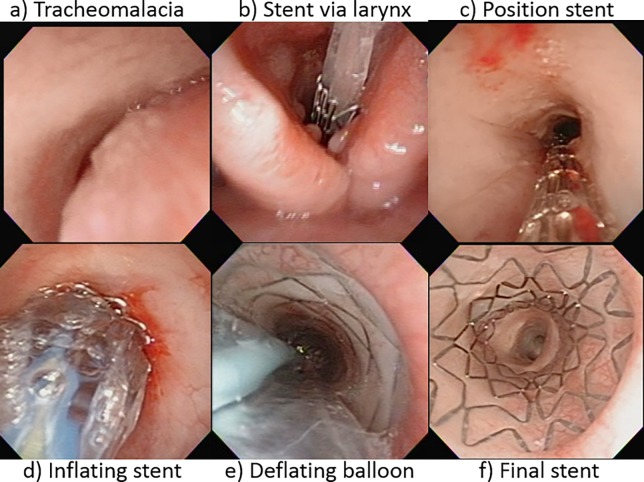
Objectives: To assess the placement, surveillance management and long-term outcomes of the tracheobronchial (TB) balloon expandable metallic stent (BEMS) managed by therapeutic flexible endoscopy (TFE).
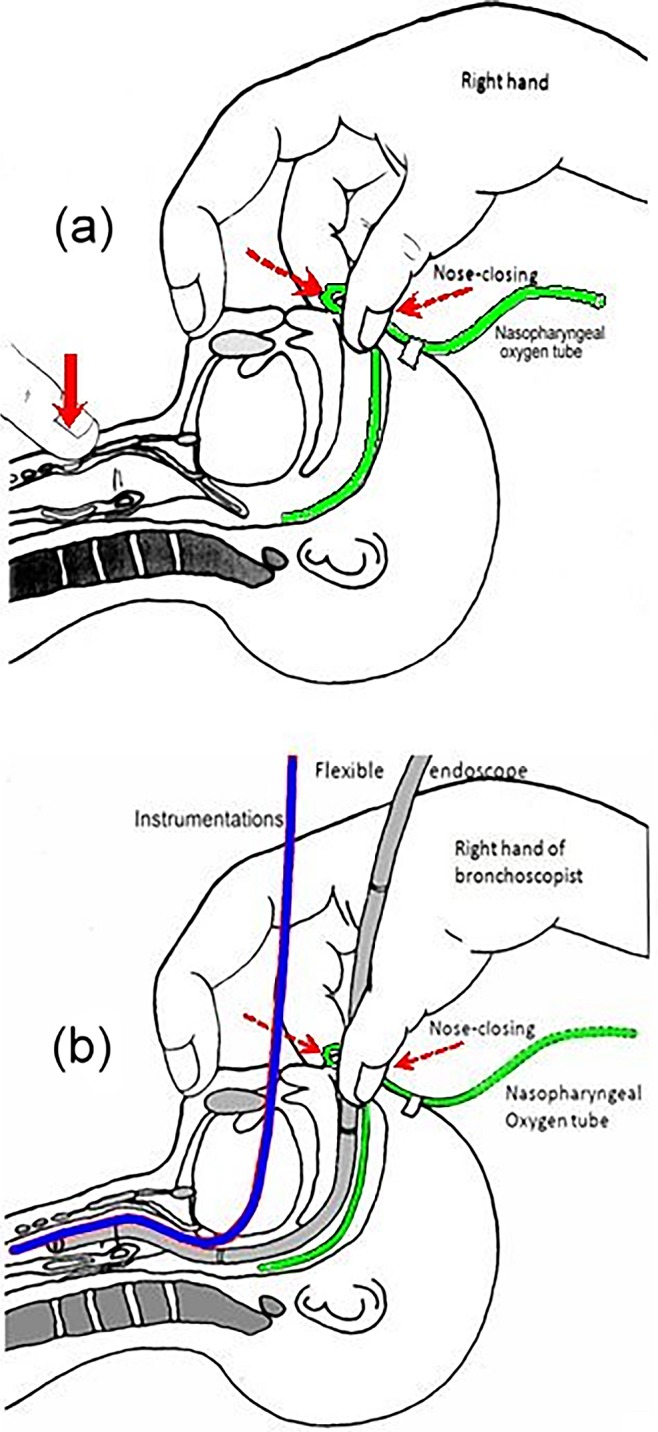
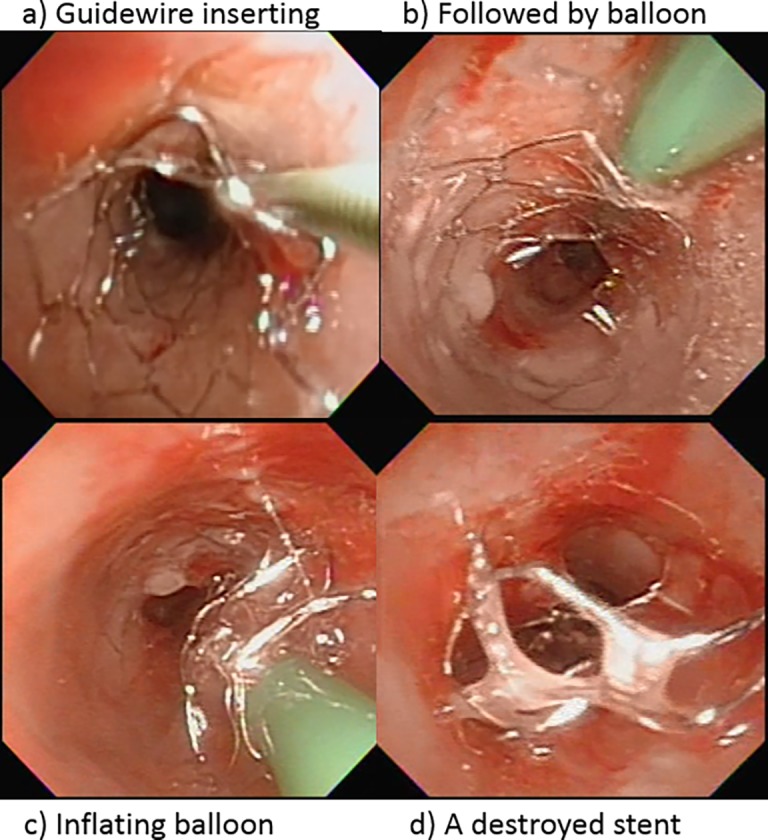
Methods: This is a retrospective review and analysis of all computerized medical records and related flexible endoscopy videos of pediatric patients who received TB BEMS during 20 years period, from January 1997 to December 2016. TFE techniques with forceps debridement, balloon dilatation and laser ablation were used to implant stents, perform regular surveillance, maintain their functions, and expand the diameters of BEMS. Short-length (30cm-36cm) endoscopes of OD 3.2mm to 5.0mm coupled with the noninvasive ventilation, without ventilation bag, mask or airway tube, supported the whole procedures.
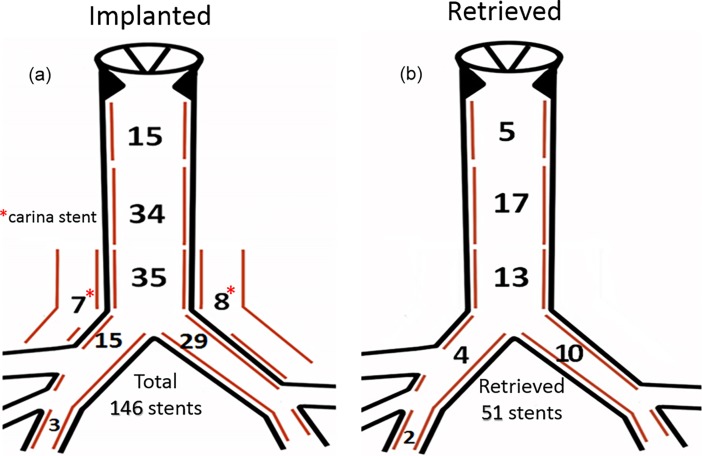
Results: 146 BEMS were implanted in 87 consecutive children, including 84 tracheal, 15 carinal and 47 bronchial stents. At the time of placement, the mean age was 35.6 ± 54.6 month-old (range 0.3-228) and the mean body weight was 13.9 ± 10.6 kg (range 2.2-60). Surveillance period was 9.4 ± 6.7 years (range, 0.3-18.0). Satisfactory clinical improvements were noted immediately in all but two patients. Seventy-two (82.8%) patients were still alive with stable respiratory status, except two patients necessitating TFE management every two months. Fifty-one stents, including 35 tracheal and 16 bronchial ones, were successfully retrieved mainly with rigid endoscopy. Implanted stents could be significantly (< .001) further expanded for growing TB lumens. The final stent diameters were positively correlated to the implanted duration. Altogether, 33 stents expired (15 patients), 51 were retrieved (40 patients), and 62 remained and functioning well (38 patients), with their mean duration of 7.4 ± 9.5, 34.9 ± 36.3 and 82.3 ± 62.5 months, respectively.
Conclusion: In pediatric patients, TFE with short-length scopes coupled with this NIV support has provided a safe, feasible and effective modality in placing and subsequently managing TB BEMS with acceptable long-term outcomes.
Conflict of interest statement
Figures



Similar articles
-
Long-term management and outcomes of tracheobronchial stent by flexible bronchoscopy in infants <5 kg: A 13-year single-center experience.J Chin Med Assoc. 2019 Sep;82(9):727-731. doi: 10.1097/JCMA.0000000000000048. J Chin Med Assoc. 2019. PMID: 30893261
-
Outcomes of Temporary Partially Covered Stent Placement for Benign Tracheobronchial Stenosis.Cardiovasc Intervent Radiol. 2016 Aug;39(8):1144-51. doi: 10.1007/s00270-016-1353-y. Epub 2016 May 4. Cardiovasc Intervent Radiol. 2016. PMID: 27146146
-
The role of airway stenting in pediatric tracheobronchial obstruction.Eur J Cardiothorac Surg. 2008 Jun;33(6):1069-75. doi: 10.1016/j.ejcts.2008.01.034. Epub 2008 Mar 4. Eur J Cardiothorac Surg. 2008. PMID: 18299200
-
Expandable metallic stents in benign tracheobronchial obstruction.J Thorac Imaging. 1998 Apr;13(2):105-15. doi: 10.1097/00005382-199804000-00005. J Thorac Imaging. 1998. PMID: 9556287 Review.
-
Stenting of the tracheobronchial tree.Radiol Clin North Am. 2000 Mar;38(2):395-408. doi: 10.1016/s0033-8389(05)70170-6. Radiol Clin North Am. 2000. PMID: 10765397 Review.
Cited by
-
Sustained pharyngeal inflation in infant airway-Flexible bronchoscopy measurements.PLoS One. 2023 Nov 22;18(11):e0294029. doi: 10.1371/journal.pone.0294029. eCollection 2023. PLoS One. 2023. PMID: 37992011 Free PMC article.
-
Flexible Endoscopy With Non-invasive Ventilation Enables Clinicians to Assess and Manage Infants With Severe Bronchopulmonary Dysplasia.Front Pediatr. 2022 Apr 19;10:837329. doi: 10.3389/fped.2022.837329. eCollection 2022. Front Pediatr. 2022. PMID: 35515350 Free PMC article.
-
Bronchial Remodeling Following Airway Stenting in Pediatric Patients With Tracheobronchial and Congenital Heart Disease.J Soc Cardiovasc Angiogr Interv. 2023 Jul 11;2(5):101068. doi: 10.1016/j.jscai.2023.101068. eCollection 2023 Sep-Oct. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39132388 Free PMC article.
-
Interventional Bronchoscopy in Children: The Way Forward.Indian J Pediatr. 2023 Aug;90(8):806-810. doi: 10.1007/s12098-023-04569-x. Epub 2023 May 20. Indian J Pediatr. 2023. PMID: 37208549 Review.
-
The use of overlapping self-expandable covered stents in the management of long-segment tracheobronchomalacia: A case report.Respirol Case Rep. 2024 Aug 10;12(8):e01451. doi: 10.1002/rcr2.1451. eCollection 2024 Aug. Respirol Case Rep. 2024. PMID: 39130087 Free PMC article.
References
-
- Filler RM, Forte V, Chait P. Tracheobronchial stenting for the treatment of airway obstruction. J Pediatr Surg 1998; 33:304–311 - PubMed
-
- Fayon M, Donato L, de Blic J, Labbé A, Becmeur F, Mely L, et al. French experience of silicone tracheobronchial stenting in children. Pediatr Pulmonol 2005; 39:21–27 doi: 10.1002/ppul.20136 - DOI - PubMed
-
- Nicolai T, Huber RM, Reiter K, Merkenschlager A, Hautmann H, Mantel K. Metal airway stent implantation in children: follow-up of seven children. Pediatr Pulmonol 2001; 31:289–296 - PubMed
-
- Furman RH, Backer CL, Dunham ME, Donaldson J, Mavroudis C, Holinger LD. The use of balloon-expandable metallic stents in the treatment of pediatric tracheomalacia and bronchomalacia. Arch Otolaryngol Head Neck Surg 1999; 125:203–207 - PubMed
-
- Antón-Pacheco JL, Cabezalí D, Tejedor R, López M, Luna C, Comas JV, et al. The role of airway stenting in pediatric tracheobronchial obstruction. Eur J Cardiothorac Surg 2008; 33:1069–1075 doi: 10.1016/j.ejcts.2008.01.034 - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
