

Stereotactic laser amygdalohippocampotomy for mesial temporal lobe epilepsy
- PMID: 29420840
- PMCID: PMC5877322
- DOI: 10.1002/ana.25180
Stereotactic laser amygdalohippocampotomy for mesial temporal lobe epilepsy
Abstract
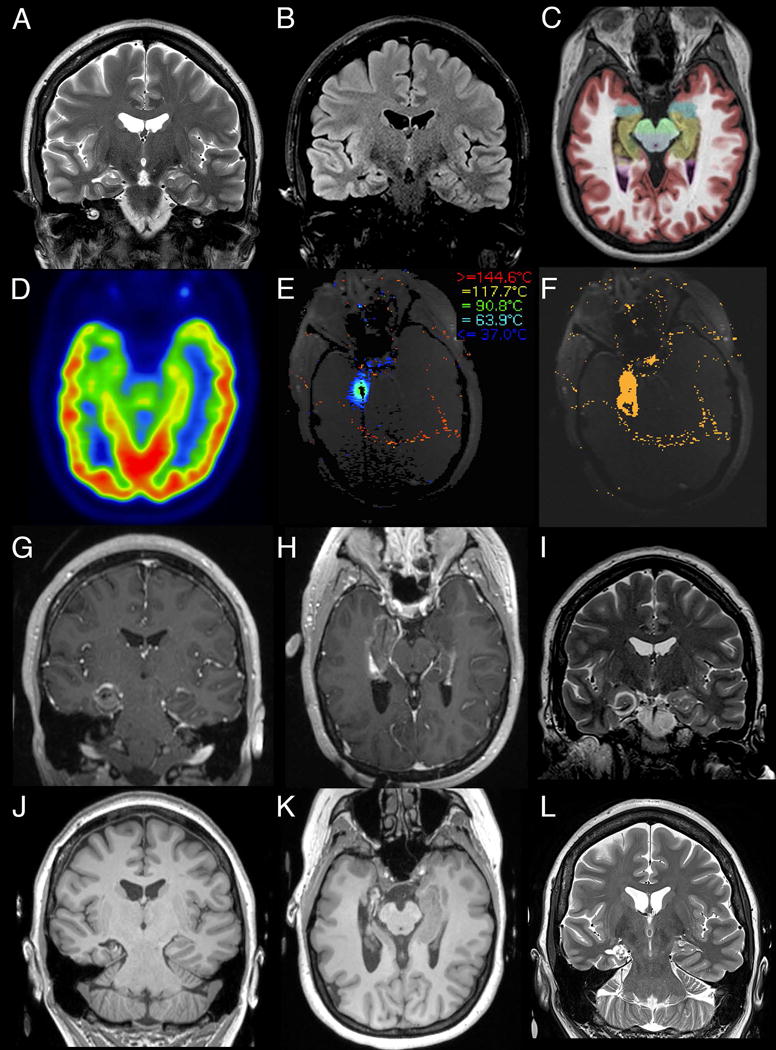
Objective: To evaluate the outcomes 1 year and longer following stereotactic laser amygdalohippocampotomy for mesial temporal lobe epilepsy in a large series of patients treated over a 5-year period since introduction of this novel technique.
Methods: Surgical outcomes of a consecutive series of 58 patients with mesial temporal lobe epilepsy who underwent the surgery at our institution with at least 12 months of follow-up were retrospectively evaluated. A subgroup analysis was performed comparing patients with and without mesial temporal sclerosis.
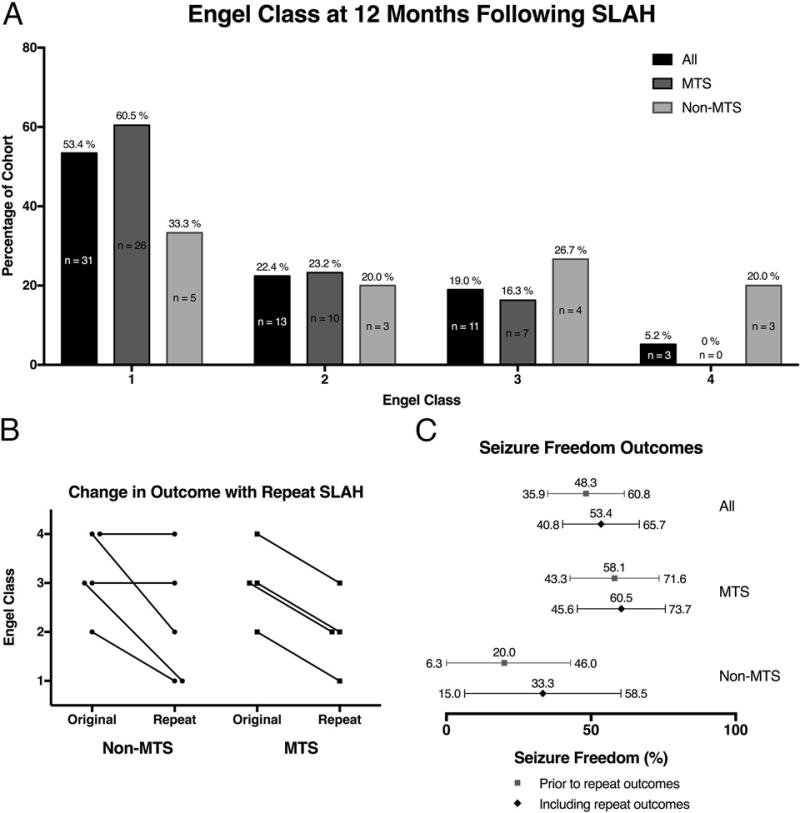
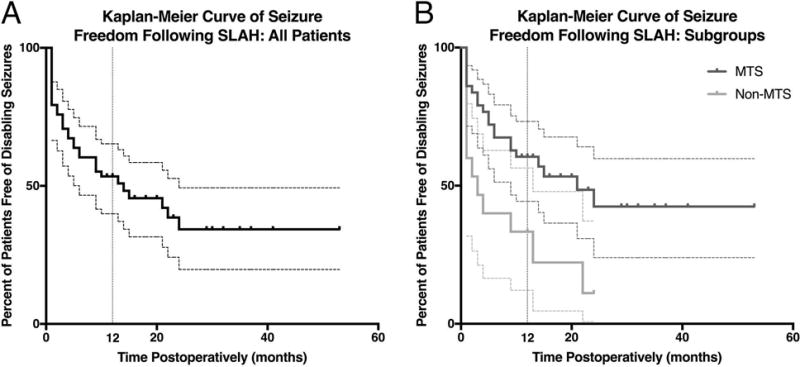
Results: One year following stereotactic laser amygdalohippocampotomy, 53.4% (95% confidence interval [CI] = 40.8-65.7%) of all patients were free of disabling seizures (Engel I). Three of 9 patients became seizure-free following repeat ablation. Subgroup analysis showed that 60.5% (95% CI = 45.6-73.7%) of patients with mesial temporal sclerosis were free of disabling seizures as compared to 33.3% (95% CI = 15.0-58.5%) of patients without mesial temporal sclerosis. Quality of Life in Epilepsy-31 scores significantly improved at the group level, few procedure-related complications were observed, and verbal memory outcome was better than historical open resection data.
Interpretation: In an unselected consecutive series of patients, stereotactic laser amygdalohippocampotomy yielded seizure-free rates for patients with mesial temporal lobe epilepsy lower than, but comparable to, the outcomes typically associated with open temporal lobe surgery. Analogous to results from open surgery, patients without mesial temporal sclerosis fared less well. This novel procedure is an effective minimally invasive alternative to resective surgery. In the minority of patients not free of disabling seizures, laser ablation presents no barrier to additional open surgery. Ann Neurol 2018;83:575-587.
© 2018 American Neurological Association.
Conflict of interest statement
RG: Dr. Gross has served as a consultant to Medtronic, Monteris, MRI interventions, Visualase, Inc., and Zimmer Biomet, which manufacture products related to the research described in this paper and may be affected by this study, and receives compensation for these services. Dr. Gross received research support from Medtronic, Inc. as part of the SLATE trial (their multisite prospective trial evaluating SLAH), and has received research grants from Visualase, Inc., and MRI Interventions. The terms of these arrangements have been reviewed and approved by Emory University in accordance with its conflict of interest policies.
JW: Dr. Willie has served as a consultant to Medtronic, Inc. and MRI Interventions, Inc., and has received compensation for these services, and receives research support from Medtronic, Inc. as part of the SLATE trial. The terms of these arrangements have been reviewed and approved by Emory University in accordance with its conflict of interest policies.
RF: Dr. Fasano receives research support from Medtronic, Inc. for the SLATE trial.
DD: Dr. Drane through Emory University has received a research grant from Medtronic, Inc., and currently serves as the core lab director for their SLATE trial. The terms of these arrangements have been reviewed and approved by Emory University in accordance with its conflict of interest policies.
Authors MS, AM, BS and NP have nothing to report.
Figures
References
-
- Hauser WA, Kurland LT. Epidemiology of epilepsy in Rochester, Minnesota, 1935 through 1967. Epilepsia. 1975;16(1):1–66. - PubMed
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M, Effectiveness Efficiency Surgery T A randomized, controlled trial of surgery for temporal-lobe epilepsy. New England Journal of Medicine. 2001 Aug 2;345(5):311–8. - PubMed
-
- Josephson CB, Dykeman J, Fiest KM, et al. Systematic review and meta-analysis of standard vs selective temporal lobe epilepsy surgery. Neurology. 2013 Apr;80(18):1669–76. - PubMed
-
- Seidenberg M, Hermann B, Wyler AR, Davies K, Dohan FC, Leveroni C. Neuropsychological outcome following anterior temporal lobectomy in patients with and without the syndrome of mesial temporal lobe epilepsy. Neuropsychology. 1998 Apr;12(2):303–16. - PubMed
-
- Spencer S, Huh L. Outcomes of epilepsy surgery in adults and children. Lancet Neurology. 2008 Jun;7(6):525–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
