

Health care and societal costs of the management of children and adolescents with attention-deficit/hyperactivity disorder in Spain: a descriptive analysis
- PMID: 29422022
- PMCID: PMC5806309
- DOI: 10.1186/s12888-017-1581-y
Health care and societal costs of the management of children and adolescents with attention-deficit/hyperactivity disorder in Spain: a descriptive analysis
Abstract
Background: Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental condition in childhood (5.3% to 7.1% worldwide prevalence), with substantial overall financial burden to children/adolescents, their families, and society. The aims of this study were to describe the clinical characteristics of children and adolescents with ADHD in Spain, estimate the associated direct/indirect costs of the disorder, and assess whether the characteristics and financial costs differed between children/adolescents adequately responding to currently available pharmacotherapies compared with children/adolescents for whom pharmacotherapies failed.
Methods: This was a multicenter, cross-sectional, descriptive analysis conducted in 15 health units representative of the overall Spanish population. Data on demographic characteristics, socio-occupational status, social relationships, clinical variables of the disease, and pharmacological and non-pharmacological treatments received were collected in 321 children and adolescents with ADHD. Direct and indirect costs were estimated over one year from both a health care system and a societal perspective.
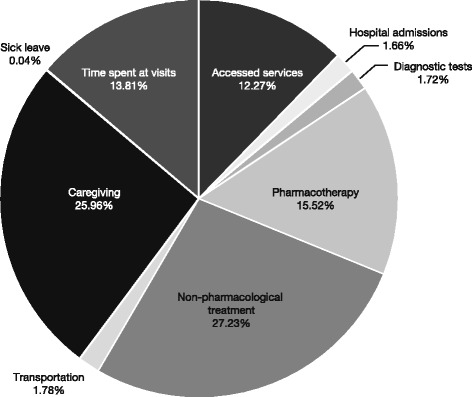
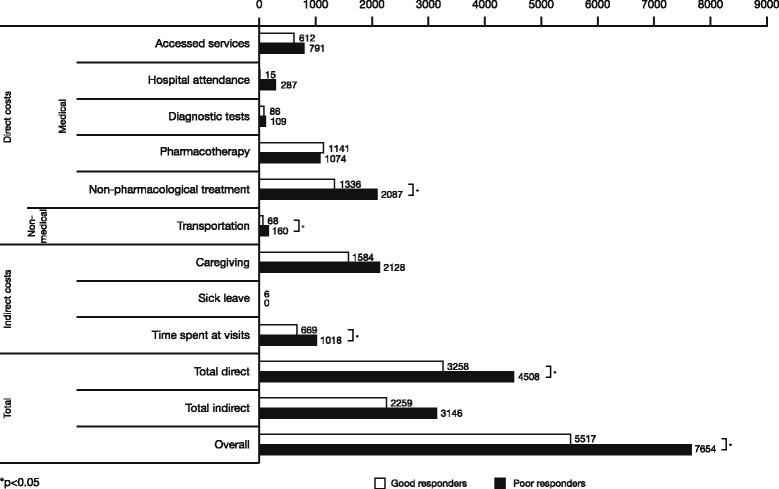
Results: The estimated average cost of ADHD per year per child/adolescent was €5733 in 2012 prices; direct costs accounted for 60.2% of the total costs (€3450). Support from a psychologist/educational psychologist represented 45.2% of direct costs and 27.2% of total costs. Pharmacotherapy accounted for 25.8% of direct costs and 15.5% of total costs. Among indirect costs (€2283), 65.2% was due to caregiver expenses. The total annual costs were significantly higher for children/adolescents who responded poorly to pharmacological treatment (€7654 versus €5517; P = 0.024), the difference being mainly due to significantly higher direct costs, particularly with larger expenses for non-pharmacological treatment (P = 0.012).
Conclusions: ADHD has a significant personal, familial, and financial impact on the Spanish health system and society. Successful pharmacological intervention was associated with lower overall expenses in the management of the disorder.
Keywords: ADHD; Adolescence; Economic evaluation; School children.
Conflict of interest statement
Ethics approval and consent to participate
The central Ethics Committee that approved the study was the Niño Jesús Hospital Committee (Madrid), and all children/adolescents and their legal representatives signed a written informed consent form prior to participation in the study.
Consent for publication
Not applicable.
Competing interests
JQ: participated as speaker and/or acted as consultant for Grunenthal, Lilly, Shire, MSD, Janssen & Ferrer; received unrestricted educational and research support from Mutua Madrileña and Otsuka. JAR-Q: on the speakers bureau and/or acted as consultant for Eli Lilly, Novartis, Shire, Lundbeck, Ferrer, Medice, and Rubió; received travel awards from Rubió, Ferrer, Shire, and Eli Lilly; received unrestricted educational and research support from Eli Lilly, Shire, Rovi, Ferrer, Lundbeck, and Rubió. FM: received funding for collaborations for congress organization from Shire, Rubió, and Rovi. AF-J: received economic support to attend courses/congresses from Janssen, Eli Lilly, Rubio, Juste, Shire, and Otsuka; received fees for participation in medical congresses from Janssen, Eli Lilly, Rubio, Juste, and Shire; participated in advisory boards for Janssen, Eli Lilly, and Shire; received grants from Janssen, Eli Lilly, Rubio, and Shire. JM-R: received honoraria for being a speaker and acting on advisory boards from Shire and Janssen Pharmaceuticals. CS: received non-personal research funds for his department from Caja Navarra Foundation, Lundbeck, Shire, and Teva; served as consultant for Alicia Koplowitz Foundation, Editorial Médica Panamericana, Eli Lilly, EUNETHYDIS, Instituto de Salud Carlos III, Medice/Juste, NeuroTech Solutions Ltd., Rubió, and Shire; served on speakers bureaux on continuous medical education for Eli Lilly, Shire, Universidad Internacional Menéndez Pelayo, and Universidad Internacional de La Rioja (UNIR); received royalties from DOYMA, Editorial Médica Panamericana, and Mayo Ediciones. MT: received grant/research support from Shire Pharmaceuticals S.L., Rubio, Rovi, and Janssen. MP: participated as speaker for Lilly, Shire, and Rovi. JC: received consulting income and research support from Janssen, Shire, Ferrer, Lilly, and Lundbeck. JS and LG-O are employees of Shire. JSS, MGG, MG, MJM, and JE received support from Shire for this research. JAA: acted as consultant to or received honoraria or grants from Eli Lilly, Shire, Janssen Cilag, Rovi, Spanish Ministry of Health, Instituto de Salud Carlos III, Agència d’Informació, Avaluació i Qualitat en Salut (AIAQS), and the Alicia Koplowitz Foundation.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Flood E, Gajria K, Sikirica V, Dietrich CN, Romero B, Harpin V, et al. The Caregiver Perspective of Paediatric ADHD (CAPPA) survey: understanding sociodemographic and clinical characteristics, treatment use, and impact of ADHD in Europe. J Affect Disord. 2016;200:222–34. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) Arlington, VA: American Psychiatric Publishing; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
