

Peak CK-MB has a strong association with chronic scar size and wall motion abnormalities after revascularized non-transmural myocardial infarction - a prospective CMR study
- PMID: 29422025
- PMCID: PMC5806273
- DOI: 10.1186/s12872-018-0767-7
Peak CK-MB has a strong association with chronic scar size and wall motion abnormalities after revascularized non-transmural myocardial infarction - a prospective CMR study
Abstract
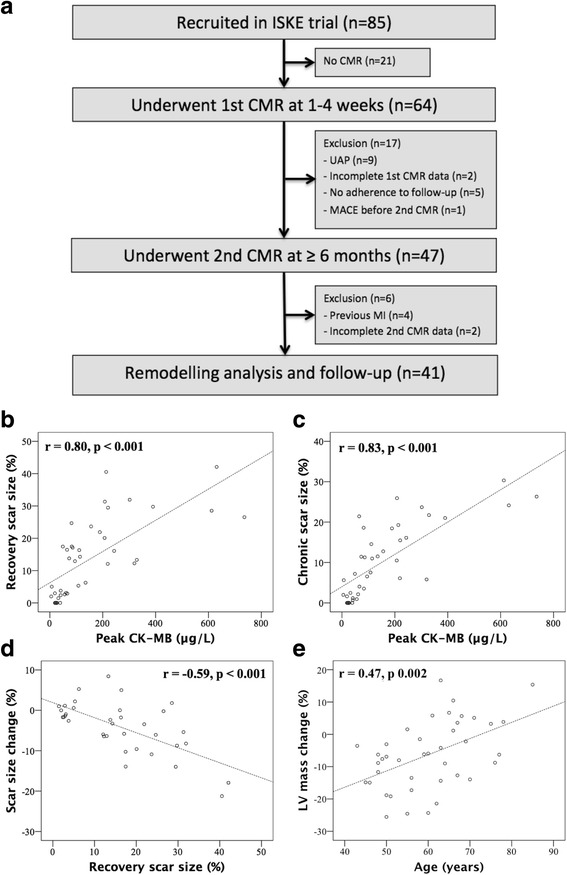
Background: Large myocardial infarction (MI) is associated with adverse left ventricular (LV) remodeling (LVR). We studied the nature of LVR, with specific attention to non-transmural MIs, and the association of peak CK-MB with recovery and chronic phase scar size and LVR.
Methods: Altogether 41 patients underwent prospectively repeated cardiovascular magnetic resonance at a median of 22 (interquartile range 9-29) days and 10 (8-16) months after the first revascularized MI. Transmural MI was defined as ≥75% enhancement in at least one myocardial segment.
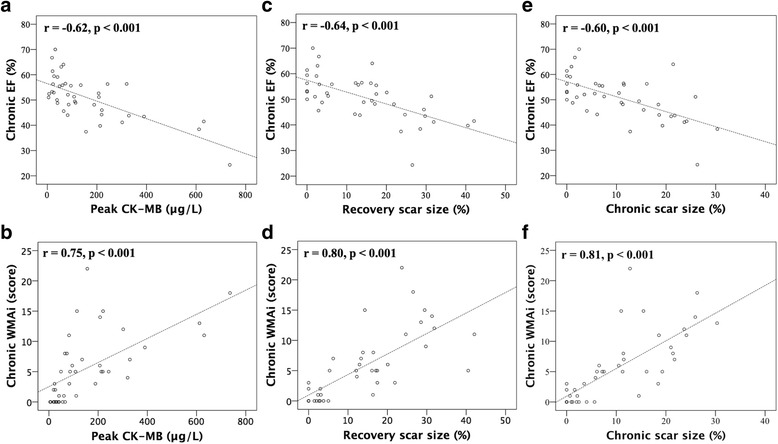
Results: Peak CK-MB was 86 (40-216) μg/L in median, while recovery and chronic phase scar size were 13 (3-23) % and 8 (2-19) %. Altogether 33 patients (81%) had a non-transmural MI. Peak CK-MB had a strong correlation with recovery and chronic scar size (r ≥ 0.80 for all, r ≥ 0.74 for non-transmural MIs; p < 0.001). Peak CK-MB, recovery scar size, and chronic scar size, were all strongly correlated with chronic wall motion abnormality index (WMAi) (r ≥ 0.75 for all, r ≥ 0.73 for non-transmural MIs; p < 0.001). There was proportional scar size and LV mass resorption of 26% (0-50%) and 6% (- 2-14%) in median. Young age (< 60 years, median) was associated with greater LV mass resorption (median 9%vs.1%, p = 0.007).
Conclusions: Peak CK-MB has a strong association with chronic scar size and wall motion abnormalities after revascularized non-transmural MI. Considerable infarct resorption happens after the first-month recovery phase. LV mass resorption is related to age, being more common in younger patients.
Keywords: Acute myocardial infarction; Cardiovascular magnetic resonance; Coronary artery disease; Creatine kinase-MB; Infarct transmurality; Left ventricular remodeling.
Conflict of interest statement
Ethics approval and consent to participate
All participants gave written informed consent and the study was approved by the ethics committee of the Helsinki University Hospital.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Infarct tissue characteristics of patients with versus without early revascularization for acute myocardial infarction: a contrast-enhancement cardiovascular magnetic resonance imaging study.Heart Vessels. 2012 May;27(3):250-7. doi: 10.1007/s00380-011-0150-4. Epub 2011 May 20. Heart Vessels. 2012. PMID: 21598029
-
The impact of infarct size on regional and global left ventricular systolic function: a cardiac magnetic resonance imaging study.Int J Cardiovasc Imaging. 2015 Jun;31(5):1037-44. doi: 10.1007/s10554-015-0657-3. Epub 2015 Apr 12. Int J Cardiovasc Imaging. 2015. PMID: 25863669
-
Coronary microvascular resistance index immediately after primary percutaneous coronary intervention as a predictor of the transmural extent of infarction in patients with ST-segment elevation anterior acute myocardial infarction.JACC Cardiovasc Imaging. 2009 Mar;2(3):263-72. doi: 10.1016/j.jcmg.2008.11.013. JACC Cardiovasc Imaging. 2009. PMID: 19356570
-
Cardiac Magnetic Resonance Evaluation of LV Remodeling Post-Myocardial Infarction: Prognosis, Monitoring and Trial Endpoints.JACC Cardiovasc Imaging. 2024 Nov;17(11):1366-1380. doi: 10.1016/j.jcmg.2024.03.012. Epub 2024 May 29. JACC Cardiovasc Imaging. 2024. PMID: 38819335 Review.
-
Risk factors for left ventricular remodeling after myocardial infarction: A meta-analysis.Medicine (Baltimore). 2024 Nov 15;103(46):e40496. doi: 10.1097/MD.0000000000040496. Medicine (Baltimore). 2024. PMID: 39560578 Free PMC article.
Cited by
-
Body fat percentage and infarct size in patients with non-ST segment elevation myocardial infarction.North Clin Istanb. 2023 Sep 13;10(5):567-574. doi: 10.14744/nci.2023.87259. eCollection 2023. North Clin Istanb. 2023. PMID: 37829751 Free PMC article.
-
Association Between Extracorporeal Cardiopulmonary Resuscitation and Prognosis in the Short and Long Term in Patients With Acute Myocardial Infarction Complicated by Refractory Cardiac Arrest.Circ Rep. 2025 Jun 11;7(7):554-561. doi: 10.1253/circrep.CR-25-0071. eCollection 2025 Jul 10. Circ Rep. 2025. PMID: 40642542 Free PMC article.
-
Rapid detection of human heart-type fatty acid-binding protein in human plasma and blood using a colloidal gold-based lateral flow immunoassay.Exp Ther Med. 2021 Nov;22(5):1238. doi: 10.3892/etm.2021.10673. Epub 2021 Aug 31. Exp Ther Med. 2021. PMID: 34539834 Free PMC article.
-
Profilin 2 and Endothelial Exosomal Profilin 2 Promote Angiogenesis and Myocardial Infarction Repair in Mice.Front Cardiovasc Med. 2022 Apr 11;9:781753. doi: 10.3389/fcvm.2022.781753. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35479278 Free PMC article.
-
The Prognostic Value of Creatine Kinase-MB Dynamics after Primary Angioplasty in ST-Elevation Myocardial Infarctions.Diagnostics (Basel). 2023 Oct 6;13(19):3143. doi: 10.3390/diagnostics13193143. Diagnostics (Basel). 2023. PMID: 37835886 Free PMC article.
References
-
- St John Sutton M, Pfeffer MA, Plappert T, Rouleau JL, Moye LA, Dagenais GR, Lamas GA, Klein M, Sussex B, Goldman S. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction. The protective effects of captopril. Circulation. 1994;89(1):68–75. doi: 10.1161/01.CIR.89.1.68. - DOI - PubMed
-
- Bolognese L, Neskovic AN, Parodi G, Cerisano G, Buonamici P, Santoro GM, Antoniucci D. Left ventricular remodeling after primary coronary angioplasty: patterns of left ventricular dilation and long-term prognostic implications. Circulation. 2002;106(18):2351–2357. doi: 10.1161/01.CIR.0000036014.90197.FA. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
