

Investigation of Adipose Tissue Fatty Acid Composition in Men with Uronephrolithiasis and Metabolic Syndrome
- PMID: 29422481
- PMCID: PMC5815268
- DOI: 10.12659/msm.906274
Investigation of Adipose Tissue Fatty Acid Composition in Men with Uronephrolithiasis and Metabolic Syndrome
Abstract
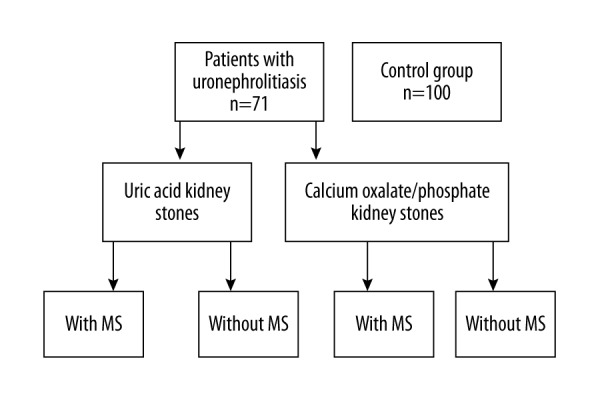
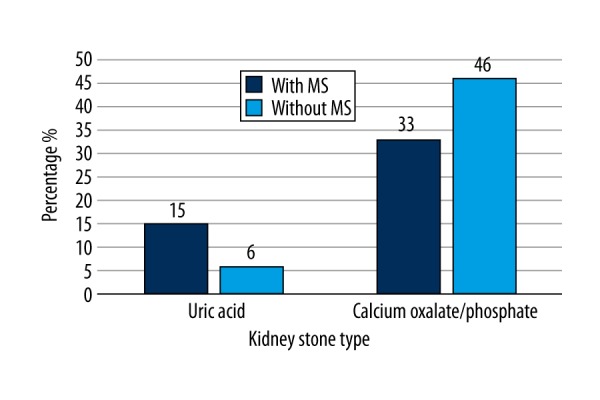
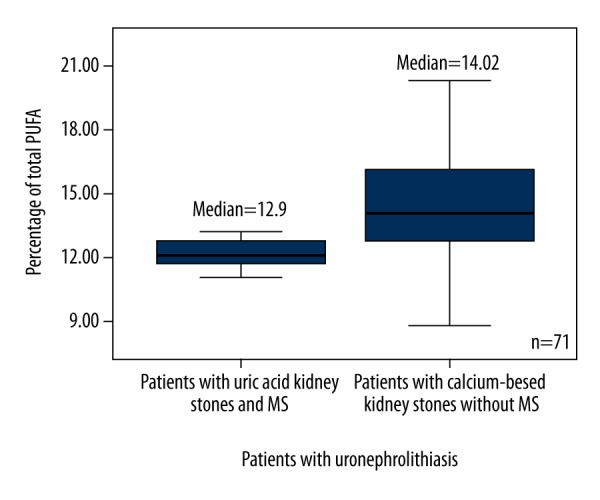
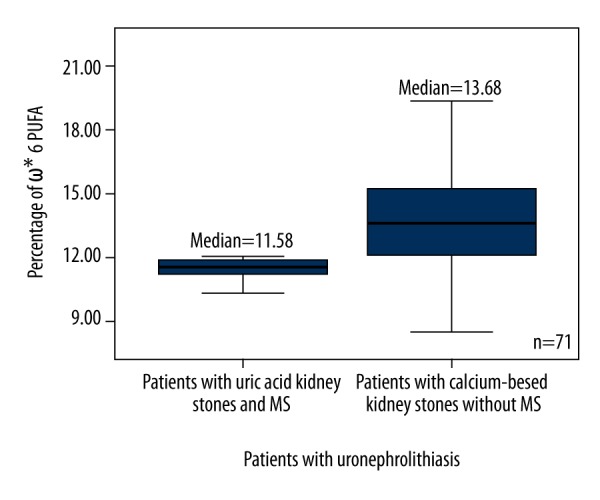
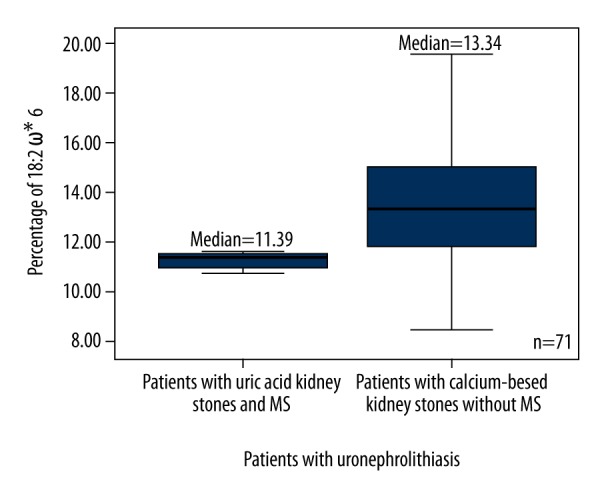
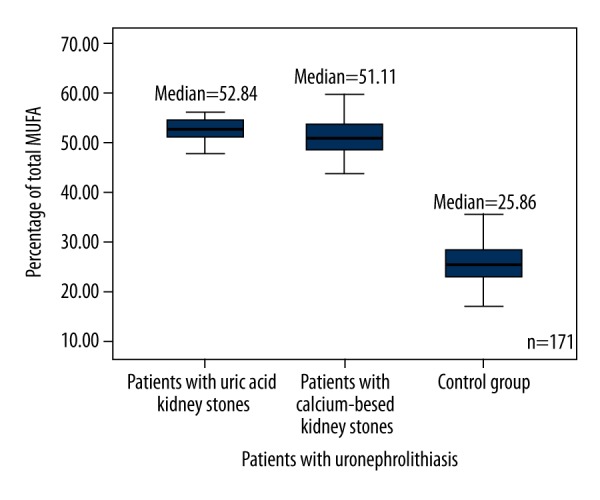
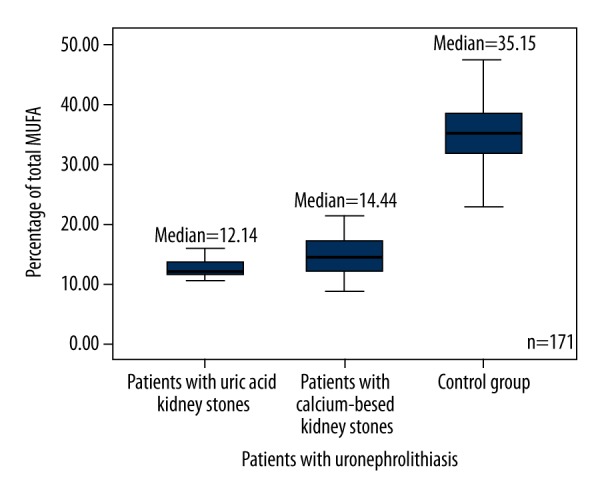
BACKGROUND Fatty acids (FA) and their metabolites are closely related to some mechanisms involved in the development of uronephrolithiasis. The aim of this study was to evaluate the relationship between FA composition and type of kidney stones. MATERIAL AND METHODS Abdominal adipose tissue fatty acid methyl esters of 71 men with nephrolithiasis were identified by GC/MS, and the type of kidney stones was identified using FTIR infrared spectroscopy. Patients were divided into groups according to diagnosis of metabolic syndrome (MS) and type of kidney stone. The composition of FA was compared within different groups of patients with different types of kidney stones and between the patients and healthy individuals (control group) (n=100). RESULTS Individuals with nephrolithiasis had a significantly higher level of monounsaturated fatty acids (MUFA) and a lower level of polyunsaturated fatty acids (PUFA) versus healthy individuals. Patients with MS had a higher level of 18: 1ω9 and a lower level of 16: 1ω7 than patients without MS. Individuals with nephrolithiasis, but without MS, had a higher level of saturated fatty acids (SFA) compared to controls. The level of PUFA was higher in the control group (p<0.0001) compared to individuals with uronephrolithiasis, with or without MS. PUFA, ω - 6 PUFA, and 18: 2ω6 were higher in patients with calcium-based kidney stones without MS versus patients with uric acid kidney stones with MS. CONCLUSIONS The levels of MUFA were significantly higher and the levels of PUFA were significantly lower in patients with uronephrolithiasis compared to controls.
Conflict of interest statement
None.
Figures
Similar articles
-
Digestion and deposition of individual fatty acids in growing-finishing pigs fed diets containing either beef tallow or sunflower oil.J Anim Physiol Anim Nutr (Berl). 2008 Aug;92(4):502-10. doi: 10.1111/j.1439-0396.2007.00741.x. Epub 2007 Nov 8. J Anim Physiol Anim Nutr (Berl). 2008. PMID: 18662360
-
The Metabolic Syndrome and the Membrane Content of Polyunsaturated Fatty Acids in Hypertensive Patients.Metab Syndr Relat Disord. 2015 Oct;13(8):343-51. doi: 10.1089/met.2015.0025. Epub 2015 Jul 23. Metab Syndr Relat Disord. 2015. PMID: 26203914
-
Association of polyunsaturated/saturated fatty acids to metabolic syndrome cardiovascular risk factors and lipoprotein (a) in hypertensive type 2 diabetic patients.Ann Biol Clin (Paris). 2017 Jun 1;75(3):293-304. doi: 10.1684/abc.2017.1244. Ann Biol Clin (Paris). 2017. PMID: 28540852 English.
-
Current Evidence Supporting the Link Between Dietary Fatty Acids and Cardiovascular Disease.Lipids. 2016 May;51(5):507-17. doi: 10.1007/s11745-015-4113-x. Epub 2015 Dec 30. Lipids. 2016. PMID: 26719191 Review.
-
Metabolic syndrome and the genesis of uric acid stones.J Ren Nutr. 2011 Jan;21(1):128-31. doi: 10.1053/j.jrn.2010.10.015. J Ren Nutr. 2011. PMID: 21195936 Free PMC article. Review.
Cited by
-
Inhibitive Effects of Huashi Pill on Formation of Renal Stones by Modulating Urine Biochemical Indexes and Osteopontin in Renal Stone Rat Models.Med Sci Monit. 2019 Nov 6;25:8335-8344. doi: 10.12659/MSM.916247. Med Sci Monit. 2019. PMID: 31690714 Free PMC article.
-
Lipidomics Reveals the Therapeutic Effects of EtOAc Extract of Orthosiphon stamineus Benth. on Nephrolithiasis.Front Pharmacol. 2020 Aug 21;11:1299. doi: 10.3389/fphar.2020.01299. eCollection 2020. Front Pharmacol. 2020. PMID: 32973524 Free PMC article.
-
Clinical Assessment of Risk Factors for Renal Atrophy After Percutaneous Nephrolithotomy.Med Sci Monit. 2020 Sep 28;26:e919970. doi: 10.12659/MSM.919970. Med Sci Monit. 2020. PMID: 32986688 Free PMC article. Clinical Trial.
-
2bRAD-M Reveals the Characteristics of Urinary Microbiota in Overweight Patients with Urinary Tract Stones.Biomedicines. 2025 May 14;13(5):1197. doi: 10.3390/biomedicines13051197. Biomedicines. 2025. PMID: 40427024 Free PMC article.
References
-
- Sakhaee K. Nephrolithiasis as a systemic disorder. Curr Opin Nephrol Hypertens. 2008;17:304–9. - PubMed
-
- Richman K, O’Bell J, Pareek G. The growing prevalence of kidney stones and opportunities for prevention. R I Med J. 2014;97(12):31–34. - PubMed
-
- Moe OW. Kidney stones: Pathophysiology and medical management. Lancet. 2006;367:333–44. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
