Immunological pathogenesis of inflammatory bowel disease
- PMID: 29422795
- PMCID: PMC5797268
- DOI: 10.5217/ir.2018.16.1.26
Immunological pathogenesis of inflammatory bowel disease
Abstract
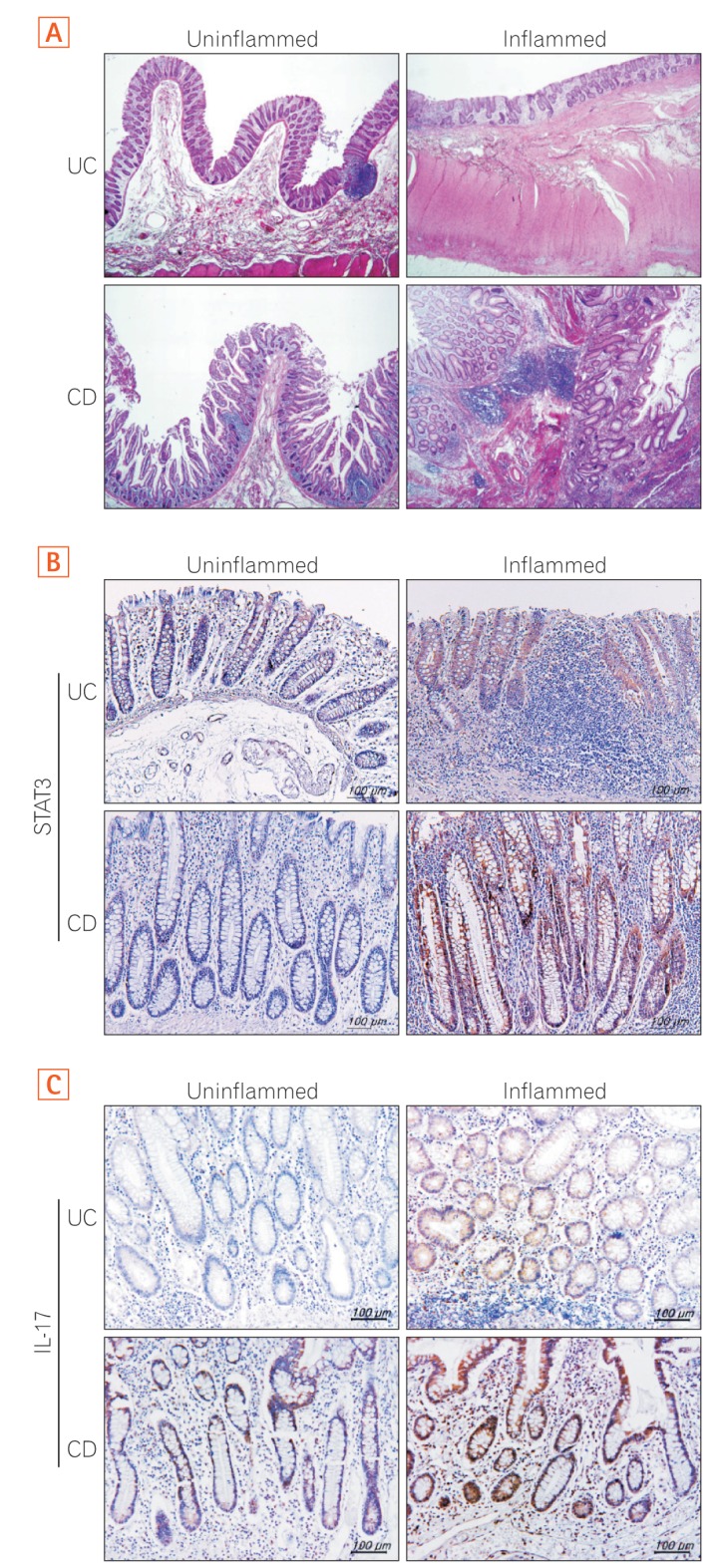
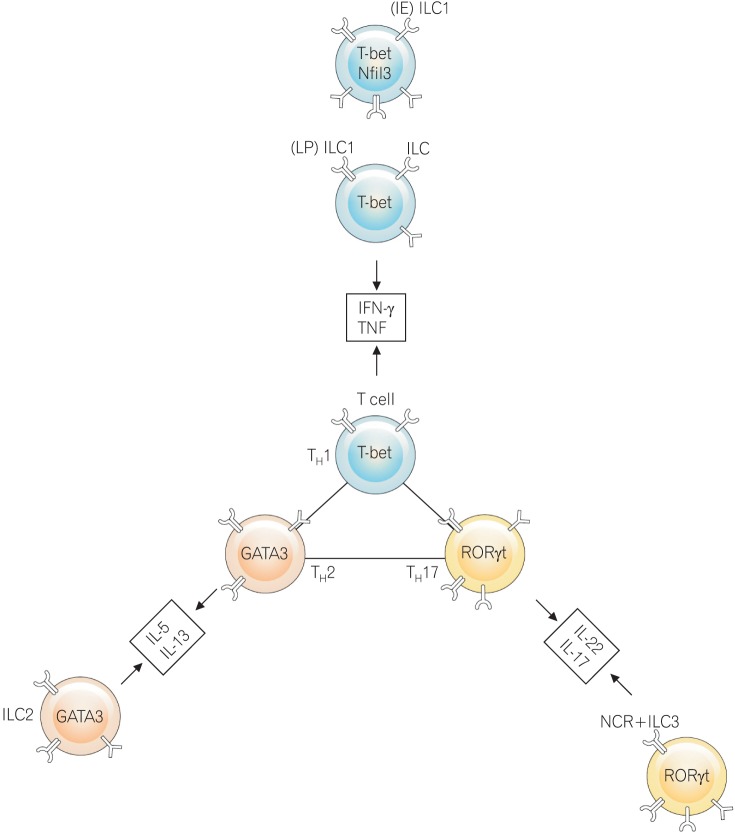
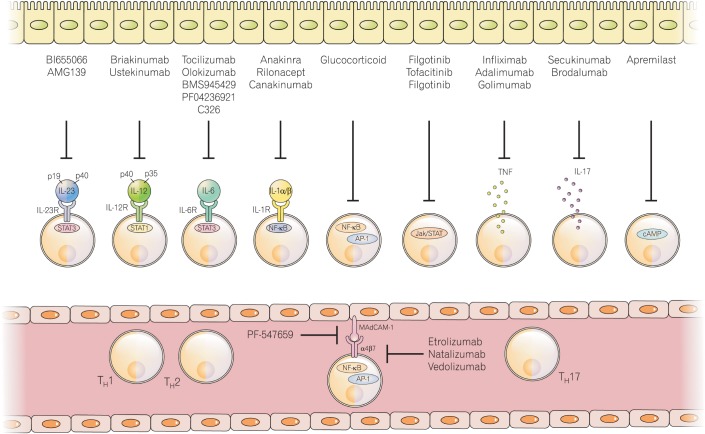
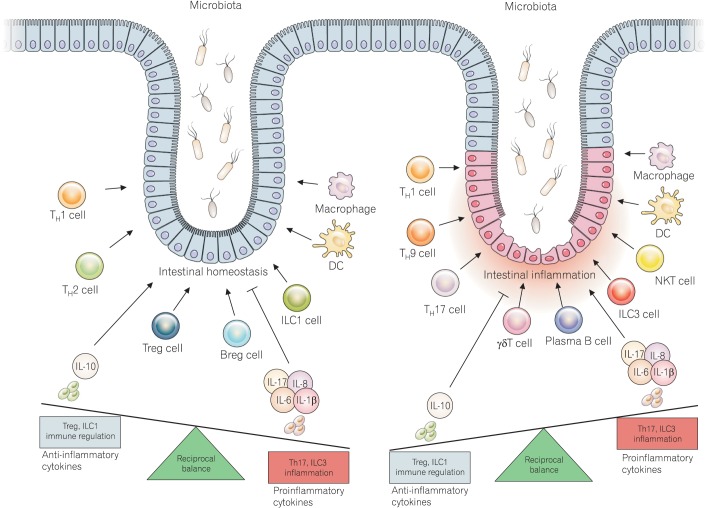
Inflammatory bowel disease (IBD) is a chronic inflammatory state of the gastrointestinal tract and can be classified into 2 main clinical phenomena: Crohn's disease (CD) and ulcerative colitis (UC). The pathogenesis of IBD, including CD and UC, involves the presence of pathogenic factors such as abnormal gut microbiota, immune response dysregulation, environmental changes, and gene variants. Although many investigations have tried to identify novel pathogenic factors associated with IBD that are related to environmental, genetic, microbial, and immune response factors, a full understanding of IBD pathogenesis is unclear. Thus, IBD treatment is far from optimal, and patient outcomes can be unsatisfactory. As result of massive studying on IBD, T helper 17 (Th17) cells and innate lymphoid cells (ILCs) are investigated on their effects on IBD. A recent study of the plasticity of Th17 cells focused primarily on colitis. ILCs also emerging as novel cell family, which play a role in the pathogenesis of IBD. IBD immunopathogenesis is key to understanding the causes of IBD and can lead to the development of IBD therapies. The aim of this review is to explain the pathogenesis of IBD, with a focus on immunological factors and therapies.
Keywords: Inflammatory bowel disease; Innate lymphoid cells; Th17 cells.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Bernstein CN, Fried M, Krabshuis JH, et al. Inflammatory bowel disease: a global perspective. Global guidelines. Milwaukee: World Gatroenterology Organization; 2009.
-
- Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet. 2007;369:1641–1657. - PubMed
-
- Leppkes M, Becker C, Ivanov II, et al. RORgamma-expressing Th17 cells induce murine chronic intestinal inflammation via redundant effects of IL-17A and IL-17F. Gastroenterology. 2009;136:257–267. - PubMed
-
- Dinarello CA. Interleukin-1beta and the autoinflammatory diseases. N Engl J Med. 2009;360:2467–2470. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials