

No neurocognitive advantage for immediate antiretroviral treatment in adults with greater than 500 CD4+ T-cell counts
- PMID: 29424786
- PMCID: PMC5920693
- DOI: 10.1097/QAD.0000000000001778
No neurocognitive advantage for immediate antiretroviral treatment in adults with greater than 500 CD4+ T-cell counts
Abstract
Objective: To compare the effect of immediate versus deferred antiretroviral treatment (ART) on neuropsychological test performance in treatment-naive HIV-positive adults with more than 500 CD4 cells/μl.
Design: Randomized trial.
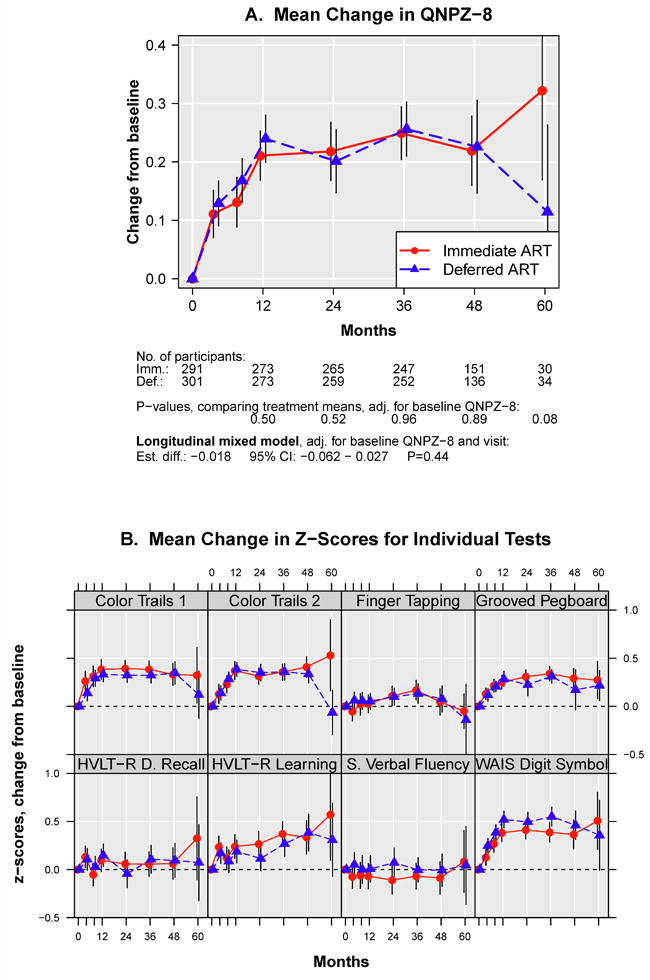
Methods: The START parent study randomized participants to commence immediate versus deferred ART until CD4 less than 350 cells/μl. The START Neurology substudy used eight neuropsychological tests, at baseline, months 4, 8, 12 and annually, to compare groups for changes in test performance. Test results were internally standardized to z-scores. The primary outcome was the average of the eight test z-scores (QNPZ-8). Mean changes in QNPZ-8 from baseline were compared by intent-to-treat using longitudinal mixed models. Changes from baseline to specific time points were compared using ANCOVA models.
Results: The 592 participants had a median age of 34 years; median baseline CD4 count was 629 cells/μl; the mean follow-up was 3.4 years. ART was used for 94 and 32% of accrued person-years in the immediate and deferred groups, respectively. There was no difference between the immediate and deferred ART groups in QNPZ-8 change through follow-up [-0.018 (95% CI -0.062 to 0.027, P = 0.44)], or at any visit. However, QNPZ-8 scores increased in both arms during the first year, by 0.22 and 0.24, respectively (P < 0.001 for increase from baseline).
Conclusion: We observed substantial improvement in neurocognitive test performance during the first year in both study arms, underlining the importance of using a control group in studies assessing neurocognitive performance over time. Immediate ART neither benefitted nor harmed neurocognitive performance in individuals with CD4 cell counts above 500 cells/μl.
Figures


References
-
- McArthur JC, Hoover DR, Bacellar H, et al. Dementia in AIDS patients: incidence and risk factors. Multicenter AIDS Cohort Study. Neurology. 1993;43(11):2245–52. - PubMed
-
- Wilkie FL, Goodkin K, Eisdorfer C, et al. Mild cognitive impairment and risk of mortality in HIV-1 infection. J Neuropsychiatry Clin Neurosci. 1998;10(2):125–32. - PubMed
-
- Albert SM, Marder K, Dooneief G, et al. Neuropsychologic impairment in early HIV infection. A risk factor for work disability. Arch Neurol. 1995;52(5):525–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
