

Allogeneic hematopoietic stem cell transplantation for relapsed follicular lymphoma: A combined analysis on behalf of the Lymphoma Working Party of the EBMT and the Lymphoma Committee of the CIBMTR
- PMID: 29424927
- PMCID: PMC5946312
- DOI: 10.1002/cncr.31264
Allogeneic hematopoietic stem cell transplantation for relapsed follicular lymphoma: A combined analysis on behalf of the Lymphoma Working Party of the EBMT and the Lymphoma Committee of the CIBMTR
Abstract
Background: Allogeneic hematopoietic stem cell transplantation (allo-HCT) remains the only potentially curative treatment option for relapsed follicular lymphoma (FL), yet questions remain about the optimal timing. This study analyzed long-term outcomes and associated factors among recipients of allo-HCT with FL.
Methods: Patients with relapsed FL who underwent allo-HCT from 2001 to 2011 with a human leukocyte antigen (HLA)-matched donor were included. Outcome analyses for overall survival (OS), progression-free survival (PFS), transplant-related mortality (TRM), and disease relapse/progression were calculated. A multivariate analysis was performed to determine factors associated with outcomes, and a prognostic score for treatment failure was developed in a subset analysis of patients.
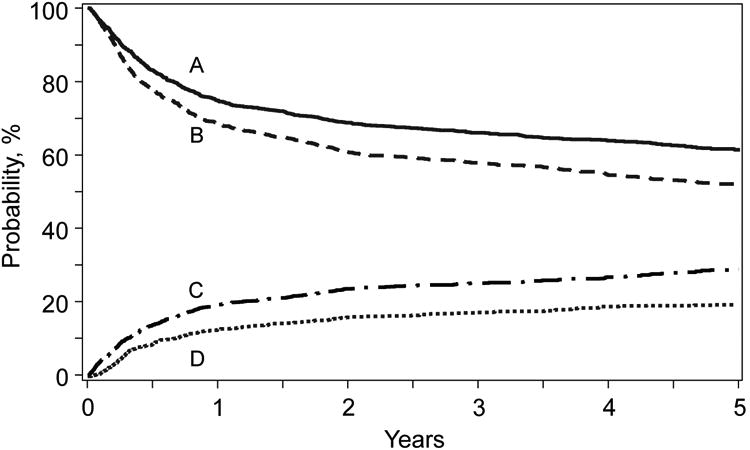
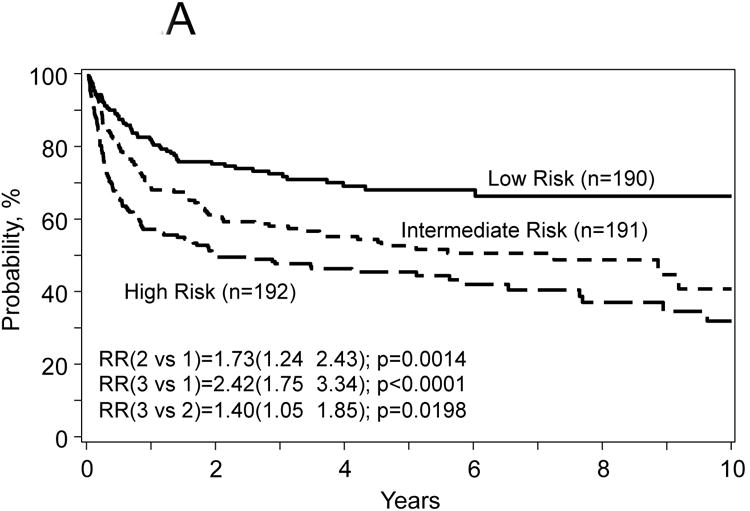
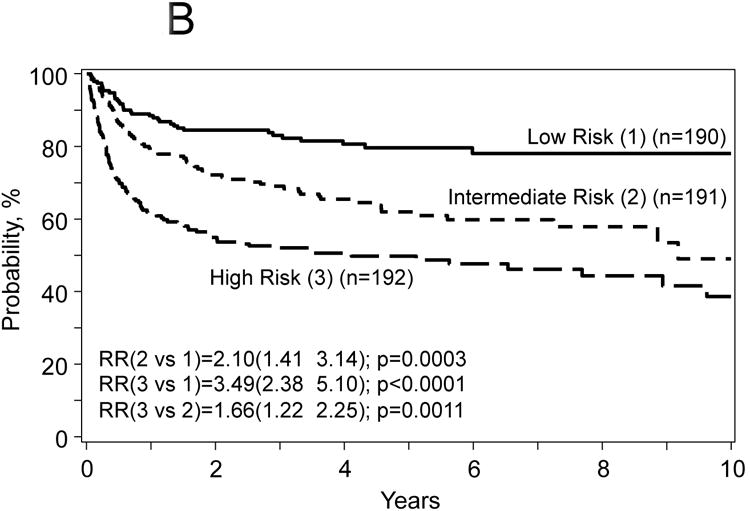
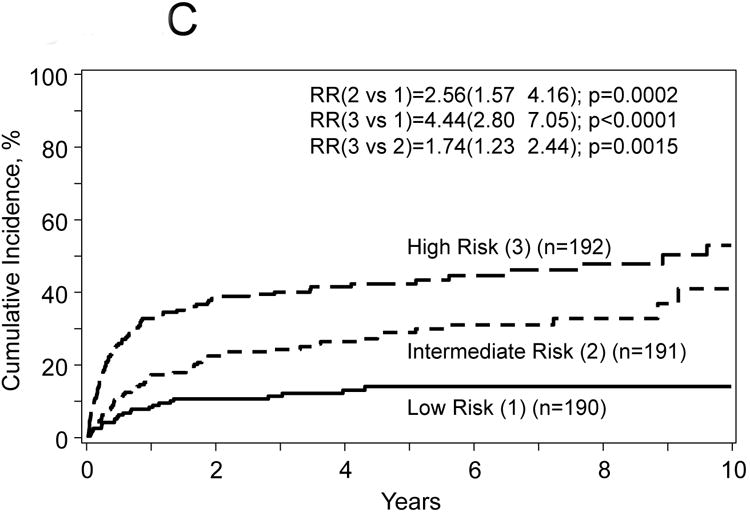
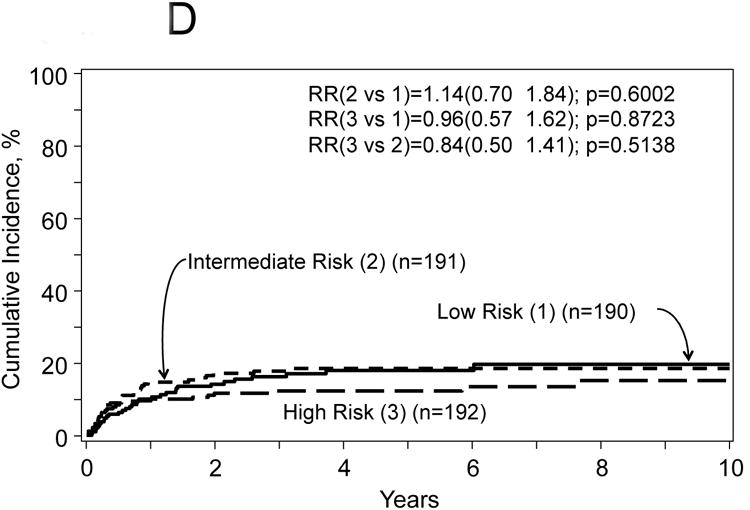
Results: In all, 1567 patients with relapsed FL were included; the median follow-up was 55 months. The 5-year probabilities of OS and PFS were 61% and 52%, respectively. The 5-year cumulative incidences of disease progression/relapse and TRM were 29% and 19%, respectively. Chemoresistant disease, older age, heavy pretreatment, poor performance status (PS), and myeloablative protocols were predictors for worse survival. The prognostic score, using age, lines of prior therapy, disease status, and PS, stratified patients into 3 groups-low, intermediate, and high risk-with 5-year PFS rates of 68%, 53%, and 46%, respectively, and 5-year OS rates of 80%, 62%, and 50%, respectively.
Conclusions: Allo-HCT should be considered for patients with relapsed FL and available HLA-matched donors. Outcomes are better in earlier phases of the disease, and reduced-intensity conditioning should be preferred. The prognostic score presented here can assist in counseling patients and determining the time to proceed to transplantation. Cancer 2018;124:1733-42. © 2018 American Cancer Society.
Keywords: allogeneic hematopoietic stem cell transplantation; follicular lymphoma; prognostic risk score; reduced-intensity conditioning protocols; unrelated donors.
© 2018 American Cancer Society.
Conflict of interest statement
Figures
Comment in
-
Reply to the persistent uncertainty of when to recommend allogeneic stem cell transplantation in follicular iymphoma.Cancer. 2018 Aug;124(16):3455-3456. doi: 10.1002/cncr.31564. Epub 2018 Jun 7. Cancer. 2018. PMID: 29878309 No abstract available.
-
The persistent uncertainty of when to recommend allogeneic stem cell transplantation in follicular iymphoma.Cancer. 2018 Aug;124(16):3454-3455. doi: 10.1002/cncr.31565. Epub 2018 Jun 7. Cancer. 2018. PMID: 29878336 No abstract available.
-
Patient selection and timing of allogeneic hematopoietic stem cell transplantation for relapsed follicular lymphoma.CA Cancer J Clin. 2018 Jul;68(4):235-236. doi: 10.3322/caac.21426. Epub 2018 Jun 21. CA Cancer J Clin. 2018. PMID: 29927482 No abstract available.
References
-
- van Besien K, Loberiza FR, Jr, Bajorunaite R, et al. Comparison of autologous and allogeneic hematopoietic stem cell transplantation for follicular lymphoma. Blood. 2003;102:3521–3529. - PubMed
-
- Robinson S, Canals C, Luang JJ, et al. The outcome of reduced intensity allogeneic stem cell transplantation and autologous stem cell transplantation when performed as a first transplant strategy in relapsed follicular lymphoma: an analysis from the Lymphoma Working Party of the EBMT. Bone Marrow Transplant. 2013;48:1409–1414. - PubMed
-
- Faulkner RD, Craddock C, Byrne JL, et al. BEAM-alemtuzumab reduced-intensity allogeneic stem cell transplantation for lymphoproliferative diseases: GVHD, toxicity, and survival in 65 patients. Blood. 2004;103:428–434. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
