

Role of the IL-23/IL-17 Axis in Psoriasis and Psoriatic Arthritis: The Clinical Importance of Its Divergence in Skin and Joints
- PMID: 29425183
- PMCID: PMC5855752
- DOI: 10.3390/ijms19020530
Role of the IL-23/IL-17 Axis in Psoriasis and Psoriatic Arthritis: The Clinical Importance of Its Divergence in Skin and Joints
Abstract
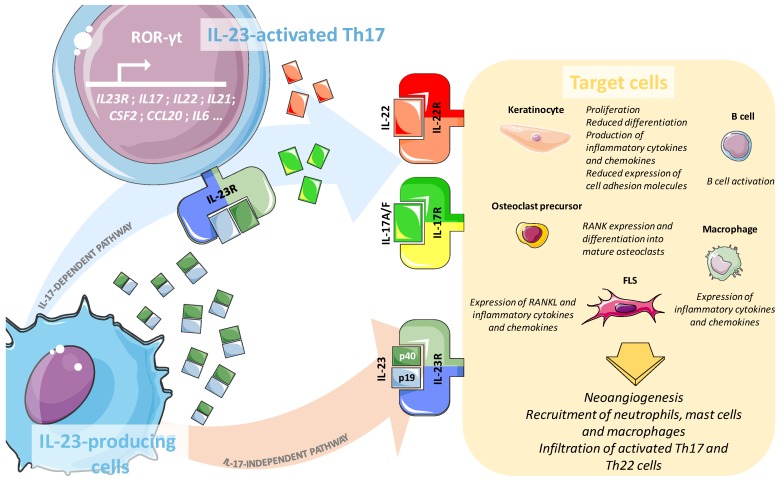
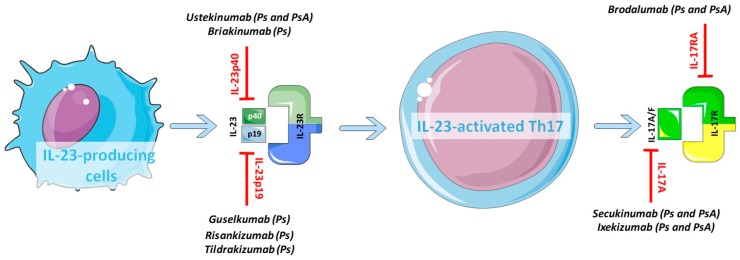
Psoriasis is a chronic systemic inflammatory disease causing erythematosus and scaly skin plaques; up to 30% of patients with psoriasis develop Psoriatic Arthritis (PsA), which is characterised by inflammation and progressive damage of the peripheral joints and/or the spine and/or the entheses. The pathogenic mechanisms driving the skin disorder in psoriasis and the joint disease in PsA are sustained by the activation of inflammatory pathways that can be overlapping, but also, at least partially, distinct. Cytokines members of the IL-23/IL-17 family, critical in the development of autoimmunity, are abundantly expressed within the cutaneous lesions but also seem to be involved in chronic inflammation and damage of the synovium though, as it will be here discussed, not in all patients. In this review, we will focus on the state of the art of the molecular features of psoriatic skin and joints, focusing on the specific role of the IL-23/IL-17 pathway in each of these anatomical districts. We will then offer an overview of the approved and in-development biologics targeting this axis, emphasising how the availability of the "target" in the diseased tissues could provide a plausible explanation for the heterogeneous clinical efficacy of these drugs, thus opening future perspective of personalised therapies.
Keywords: Th17 cells; interleukin-17; interleukine-23; psoriasis; psoriatic arthritis.
Conflict of interest statement
The authors declare no conflict of interest. The funding sponsors had no role in the writing of the manuscript and in the decision to publish this review.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
