

Evidence of previous but not current transmission of chikungunya virus in southern and central Vietnam: Results from a systematic review and a seroprevalence study in four locations
- PMID: 29425199
- PMCID: PMC5823466
- DOI: 10.1371/journal.pntd.0006246
Evidence of previous but not current transmission of chikungunya virus in southern and central Vietnam: Results from a systematic review and a seroprevalence study in four locations
Abstract
Background: Arbovirus infections are a serious concern in tropical countries due to their high levels of transmission and morbidity. With the outbreaks of chikungunya (CHIKV) in surrounding regions in recent years and the fact that the environment in Vietnam is suitable for the vectors of CHIKV, the possibility of transmission of CHIKV in Vietnam is of great interest. However, information about CHIKV activity in Vietnam remains limited.
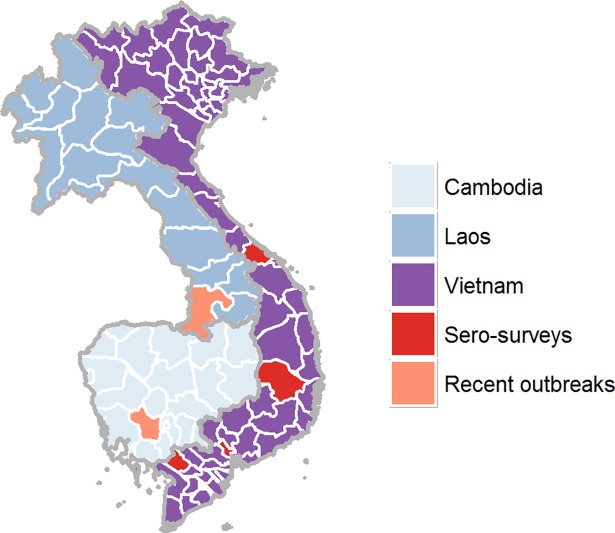
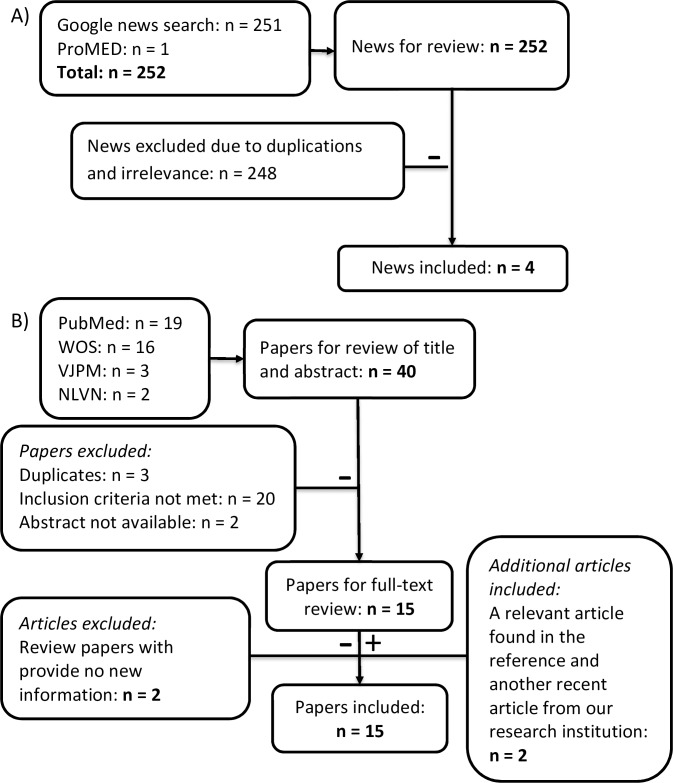
Methodology: In order to address this question, we performed a systematic review of CHIKV in Vietnam and a CHIKV seroprevalence survey. The seroprevalence survey tested for CHIKV IgG in population serum samples from individuals of all ages in 2015 from four locations in Vietnam.
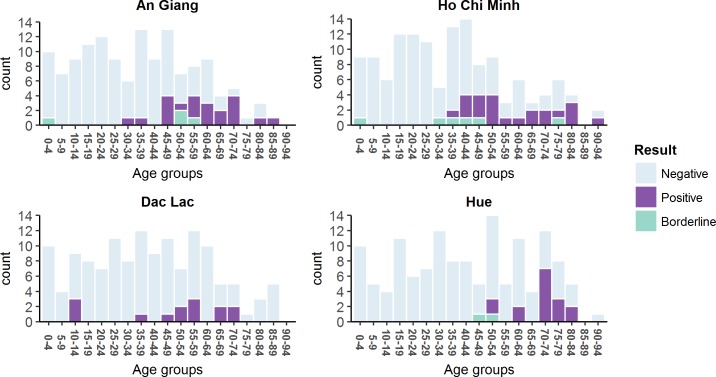
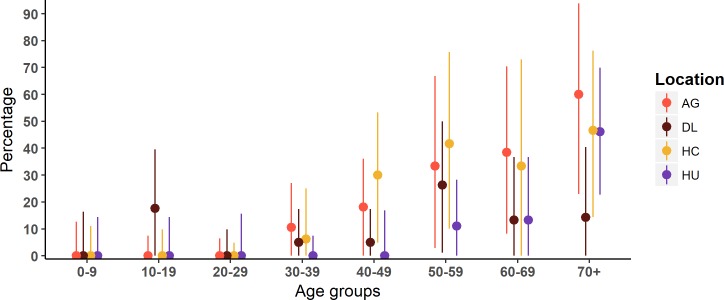
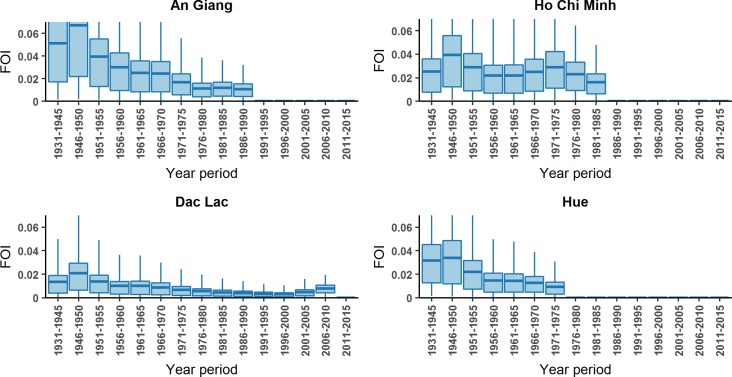
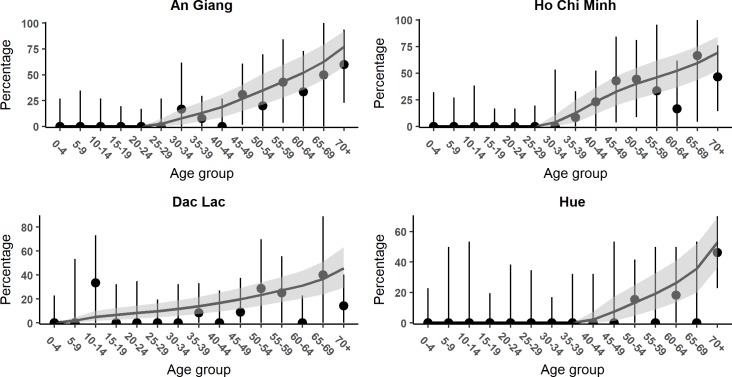
Principal findings: The four locations were An Giang province (n = 137), Ho Chi Minh City (n = 136), Dak Lak province (n = 137), and Hue City (n = 136). The findings give us evidence of some CHIKV activity: 73/546 of overall samples were seropositive (13.4%). The age-adjusted seroprevalences were 12.30% (6.58-18.02), 13.42% (7.16-19.68), 7.97% (3.56-12.38), and 3.72% (1.75-5.69) in An Giang province, Ho Chi Minh City, Dak Lak province, and Hue City respectively. However, the age-stratified seroprevalence suggests that the last transmission ended around 30 years ago, consistent with results from the systematic review. We see no evidence for on-going transmission in three of the locations, though with some evidence of recent exposure in Dak Lak, most likely due to transmission in neighbouring countries. Before the 1980s, when transmission was occurring, we estimate on average 2-4% of the population were infected each year in HCMC and An Giang and Hue (though transmision ended earlier in Hue). We estimate lower transmission in Dak Lak, with around 1% of the population infected each year.
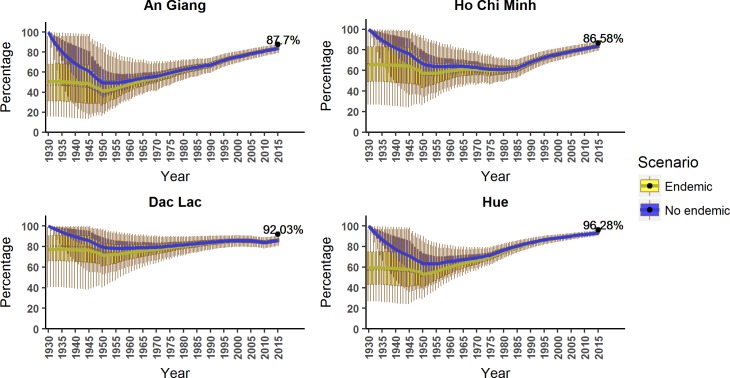
Conclusion: In conclusion, we find evidence of past CHIKV transmission in central and southern Vietnam, but no evidence of recent sustained transmission. When transmission of CHIKV did occur, it appeared to be widespread and affect a geographically diverse population. The estimated susceptibility of the population to chikungunya is continually increasing, therefore the possibility of future CHIKV transmission in Vietnam remains.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- CDC- Division of Vector-Borne Diseases. Revised diagnostic testing for Zika, chikungunya, and dengue viruses in US Public Health Laboratories. Available from: https://www.cdc.gov/zika/pdfs/denvchikvzikv-testing-algorithm.pdf.
-
- Hoarau J-J, Bandjee M-CJ, Trotot PK, Das T, Li-Pat-Yuen G, Dassa B, et al. Persistent chronic inflammation and infection by Chikungunya arthritogenic alphavirus in spite of a robust host immune response. The Journal of Immunology. 2010;184(10):5914–27. doi: 10.4049/jimmunol.0900255 - DOI - PubMed
-
- Sissoko D, Malvy D, Ezzedine K, Renault P, Moscetti F, Ledrans M, et al. Post-epidemic Chikungunya disease on Reunion Island: course of rheumatic manifestations and associated factors over a 15-month period. PLoS Negl Trop Dis. 2009;3(3):e389 doi: 10.1371/journal.pntd.0000389 - DOI - PMC - PubMed
-
- Gasque P, Couderc T, Lecuit M, Roques P, Ng LF. Chikungunya virus pathogenesis and immunity. Vector borne and zoonotic diseases (Larchmont, NY). 2015;15(4):241–9. - PubMed
-
- Moro ML, Gagliotti C, Silvi G, Angelini R, Sambri V, Rezza G, et al. Chikungunya virus in North-Eastern Italy: a seroprevalence survey. The American journal of tropical medicine and hygiene. 2010;82(3):508–11. doi: 10.4269/ajtmh.2010.09-0322 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
