

Impact and cost-effectiveness of different vaccination strategies to reduce the burden of pneumococcal disease among elderly in the Netherlands
- PMID: 29425249
- PMCID: PMC5806887
- DOI: 10.1371/journal.pone.0192640
Impact and cost-effectiveness of different vaccination strategies to reduce the burden of pneumococcal disease among elderly in the Netherlands
Abstract
Background: Streptococcus pneumoniae causes morbidity and mortality among all ages in The Netherlands. To reduce this burden, infants in The Netherlands receive the 10-valent pneumococcal conjugated vaccine (PCV10), but older persons are not targeted. We assessed the impact and cost-effectiveness of vaccination with 23-valent pneumococcal polysaccharide vaccine (PPV23) or 13-valent PCV (PCV13) among all those aged 60, 65 or 70 and/or in combination with replacing PCV10 with PCV13 in the infant vaccination programme.
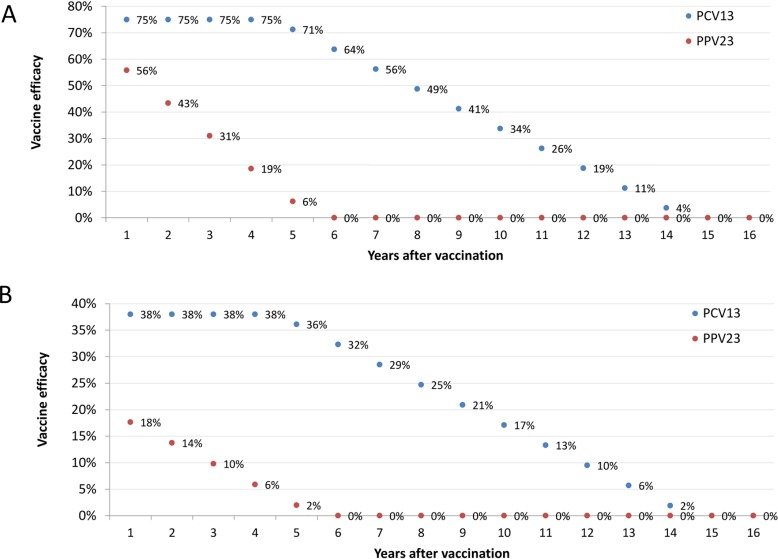
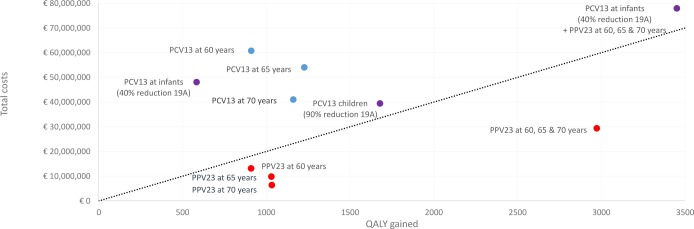
Methods: A static cost-effectiveness model was parameterized including projected trends for invasive pneumococcal disease (IPD) and hospitalised community acquired pneumonia (CAP). The different strategies were evaluated using vaccine list prices and a 10-year time horizon. Incremental cost-effectiveness ratios (ICER) were calculated with the current strategy (infant vaccination program with PCV10) as reference.
Results: Compared to the reference, the largest impact on pneumococcal disease burden was projected with a combined use of PCV13 among infants and PPV23 at 60, 65 and 70 years, preventing 1,635 cases of IPD and 914 cases of CAP. The most cost-effective strategy was vaccinating with PPV23 at 70 years only with similar low ICERs at age 60 and 65. The impact of the use of PCV13 among infants depends strongly on the projected herd-immunity effect on serotype 19A. Vaccinating elderly with either PCV13 or PPV23 was dominated by PPV23 in all investigated scenarios, mainly due to the lower price of PPV23.
Conclusion: Under the current assumptions, the best value for money is the use of PPV23 for elderly, with a single dose or at five year increment between age 60 to age 70.
Conflict of interest statement
Figures

Similar articles
-
Cost-effectiveness of 13-valent pneumococcal conjugate vaccine (PCV13) in older Australians.Vaccine. 2017 Aug 3;35(34):4307-4314. doi: 10.1016/j.vaccine.2017.06.085. Epub 2017 Jul 8. Vaccine. 2017. PMID: 28693751
-
Retrospective cost-effectiveness of the 23-valent pneumococcal polysaccharide vaccination program in Australia.Vaccine. 2018 Oct 8;36(42):6307-6313. doi: 10.1016/j.vaccine.2018.08.084. Epub 2018 Sep 10. Vaccine. 2018. PMID: 30213457
-
The impact and cost-effectiveness of pneumococcal immunisation strategies for the elderly in England.Vaccine. 2024 Jul 11;42(18):3838-3850. doi: 10.1016/j.vaccine.2024.05.001. Epub 2024 May 18. Vaccine. 2024. PMID: 38763851
-
Systematic review of economic evaluations of the 23-valent pneumococcal polysaccharide vaccine (PPV23) in individuals 60 years of age or older.Vaccine. 2018 May 3;36(19):2510-2522. doi: 10.1016/j.vaccine.2018.03.070. Epub 2018 Apr 2. Vaccine. 2018. PMID: 29618414
-
Cost Effectiveness of Elderly Pneumococcal Vaccination in Presence of Higher-Valent Pneumococcal Conjugate Childhood Vaccination: Systematic Literature Review with Focus on Methods and Assumptions.Pharmacoeconomics. 2019 Sep;37(9):1093-1127. doi: 10.1007/s40273-019-00805-5. Pharmacoeconomics. 2019. PMID: 31025189
Cited by
-
Estimating the Impact of Switching from a Lower to Higher Valent Pneumococcal Conjugate Vaccine in Colombia, Finland, and The Netherlands: A Cost-Effectiveness Analysis.Infect Dis Ther. 2020 Jun;9(2):305-324. doi: 10.1007/s40121-020-00287-5. Epub 2020 Feb 24. Infect Dis Ther. 2020. PMID: 32096144 Free PMC article.
-
State-of-the-art in the pneumococcal field: Proceedings of the 11th International Symposium on Pneumococci and Pneumococcal Diseases (ISPPD-11).Pneumonia (Nathan). 2020 Feb 5;12:2. doi: 10.1186/s41479-019-0064-y. eCollection 2020. Pneumonia (Nathan). 2020. PMID: 32042572 Free PMC article. Review.
-
Modeling the sustained use of the 13-valent pneumococcal conjugate vaccine compared to switching to the 10-valent vaccine in Mexico.Hum Vaccin Immunother. 2019;15(3):560-569. doi: 10.1080/21645515.2018.1516491. Epub 2018 Sep 21. Hum Vaccin Immunother. 2019. PMID: 30156978 Free PMC article.
-
Cost-effectiveness and budget impact analysis of PPV23 vaccination for the Malaysian Hajj pilgrims.PLoS One. 2022 Jan 24;17(1):e0262949. doi: 10.1371/journal.pone.0262949. eCollection 2022. PLoS One. 2022. PMID: 35073385 Free PMC article.
-
Response to McGirr et al.'s Comment on "Clinical and Economic Impact of a Potential Switch from 13-Valent to 10-Valent Pneumococcal Conjugate Infant Vaccination in Canada".Infect Dis Ther. 2018 Dec;7(4):539-543. doi: 10.1007/s40121-018-0221-2. Epub 2018 Nov 8. Infect Dis Ther. 2018. PMID: 30411203 Free PMC article. No abstract available.
References
-
- O’Brien KL, Wolfson LJ, Watt JP, Henkle E, Deloria-Knoll M, McCall N, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. Elsevier Ltd; 2009;374: 893–902. doi: 10.1016/S0140-6736(09)61204-6 - DOI - PubMed
-
- Fedson DS, Scott J a, Scott G. The burden of pneumococcal disease among adults in developed and developing countries: what is and is not known. Vaccine. 1999;17 Suppl 1: S11–8. Available: http://www.ncbi.nlm.nih.gov/pubmed/10471174 - PubMed
-
- RIVM. LCI Guideline [Internet]. 2017 [cited 5 Oct 2017]. Available: https://lci.rivm.nl/richtlijnen/pneumokokkenziekte-invasief
-
- Wagenvoort GHJ, Sanders EAM, Vlaminckx BJ, Elberse KE, de Melker HE, van der Ende A, et al. Invasive pneumococcal disease: Clinical outcomes and patient characteristics 2–6 years after introduction of 7-valent pneumococcal conjugate vaccine compared to the pre-vaccine period, the Netherlands. Vaccine. Elsevier Ltd; 2016;34: 1077–1085. doi: 10.1016/j.vaccine.2015.12.066 - DOI - PubMed
-
- Knol MJ, Wagenvoort GHJ, Sanders EAM, Elberse K, Vlaminckx BJ, de Melker HE, et al. Invasive Pneumococcal Disease 3 Years after Introduction of 10-Valent Pneumococcal Conjugate Vaccine, the Netherlands. Emerg Infect Dis. 2015;21: 2040–4. doi: 10.3201/eid2111.140780 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
