

Clinical effectiveness of care managers in collaborative care for patients with depression in Swedish primary health care: a pragmatic cluster randomized controlled trial
- PMID: 29426288
- PMCID: PMC5807835
- DOI: 10.1186/s12875-018-0711-z
Clinical effectiveness of care managers in collaborative care for patients with depression in Swedish primary health care: a pragmatic cluster randomized controlled trial
Abstract
Background: Depression is one of the leading causes of disability and affects 10-15% of the population. The majority of people with depressive symptoms seek care and are treated in primary care. Evidence internationally for high quality care supports collaborative care with a care manager. Our aim was to study clinical effectiveness of a care manager intervention in management of primary care patients with depression in Sweden.
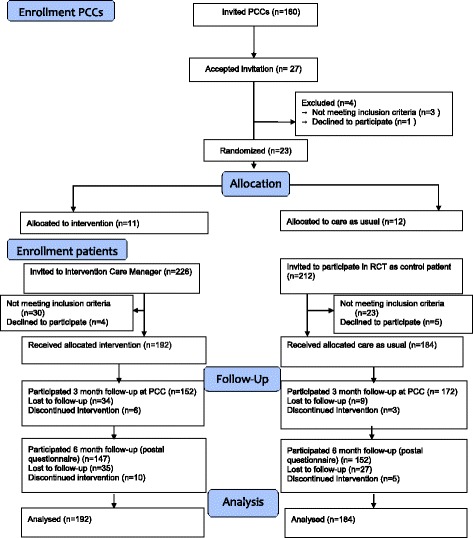
Methods: In a pragmatic cluster randomized controlled trial 23 primary care centers (PCCs), urban and rural, included patients aged ≥ 18 years with a new (< 1 month) depression diagnosis. Intervention consisted of Care management including continuous contact between care manager and patient, a structured management plan, and behavioral activation, altogether around 6-7 contacts over 12 weeks. Control condition was care as usual (CAU).
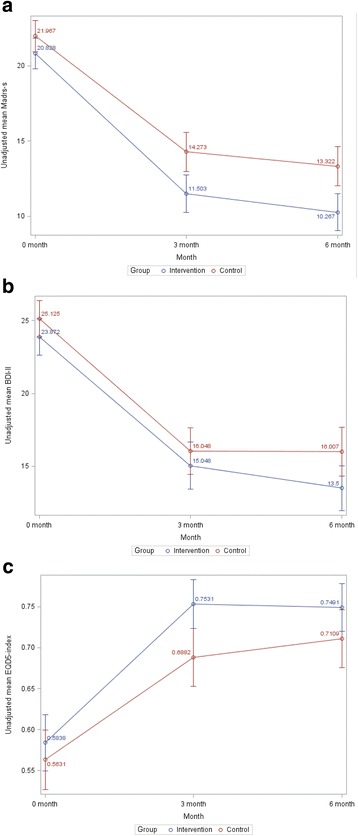
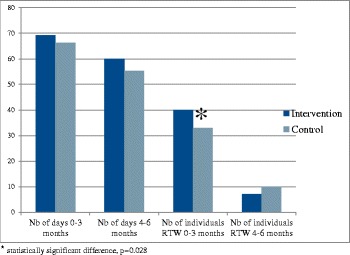
Outcome measures: Depression symptoms (measured by Mongomery-Asberg depression score-self (MADRS-S) and BDI-II), quality of life (QoL) (EQ-5D), return to work and sick leave, service satisfaction, and antidepressant medication. Data were analyzed with the intention-to-treat principle.
Results: One hundred ninety two patients with depression at PCCs with care managers were allocated to the intervention group, and 184 patients at control PCCs were allocated to the control group. Mean depression score measured by MADRS-S was 2.17 lower in the intervention vs. the control group (95% CI [0.56; 3.79], p = 0.009) at 3 months and 2.27 lower (95% CI [0.59; 3.95], p = 0.008) at 6 months; corresponding BDI-II scores were 1.96 lower (95% CI [- 0.19; 4.11], p = 0.07) in the intervention vs. control group at 6 months. Remission was significantly higher in the intervention group at 6 months (61% vs. 47%, p = 0.006). QoL showed a steeper increase in the intervention group at 3 months (p = 0.01). During the first 3 months, return to work was significantly higher in the intervention vs. the control group. Patients in the intervention group were more consistently on antidepressant medication than patients in the control group.
Conclusions: Care managers for depression treatment have positive effects on depression course, return to work, remission frequency, antidepressant frequency, and quality of life compared to usual care and is valued by the patients.
Trial registration: Identifier: NCT02378272 . February 2, 2015. Retrospectively registered.
Keywords: Care manager; Collaborative care; Depression; Primary care; Quality-of- life; Sick-leave.
Conflict of interest statement
Ethics approval and consent to participate
The Regional Ethical Review Board in Gothenburg, Sweden approved this study (Dnr 903-13; January 2, 2014; complementary approval for Dalarna January 7, 2015 (T975-14)).
Consent to participate: Prior to inclusion and after receiving oral and written information about the study, participants provided written informed consent.
Written permission for conduct of study was obtained from the head of the regional primary care health authority and all participating PCCs, which includes conduct of personnel at the PCCs. Oral informed consent was also obtained from GPs and nurses at the participating PCCs.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Swedish Council on Health Technology Assessment. Treatment of depressive disorders – a literature review. Report 166. Stockholm: 2004. p. 1.
-
- WHO. Methods and data sources for global burden of disease estimates 2000-2011. Geneva: WHO; 2013. http://www.who.int/healthinfo/statistics/GlobalDALYmethods_2000_2011.pdf. Accessed 25 May 2017.
-
- National Guidelines for depression and anxiety syndromes. The Swedish National Board of Health and Welfare. Stockholm; 2010. http://www.angest-stockholm.se/wp-content/uploads/2009/08/Socialstyrelse.... Accessed 27 Jan 2018.
-
- Månsson J, Nilsson G, Strender LE, Björkelund C. Reasons for encounters, investigations, referrals, diagnoses and treatments in general practice in Sweden--a multicentre pilot study using electronic patient records. Euro J Gen Pract. 2011;17(2):87–94. doi: 10.3109/13814788.2010.538675. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
