

Poly-arginine R18 and R18D (D-enantiomer) peptides reduce infarct volume and improves behavioural outcomes following perinatal hypoxic-ischaemic encephalopathy in the P7 rat
- PMID: 29426351
- PMCID: PMC5810179
- DOI: 10.1186/s13041-018-0352-0
Poly-arginine R18 and R18D (D-enantiomer) peptides reduce infarct volume and improves behavioural outcomes following perinatal hypoxic-ischaemic encephalopathy in the P7 rat
Abstract
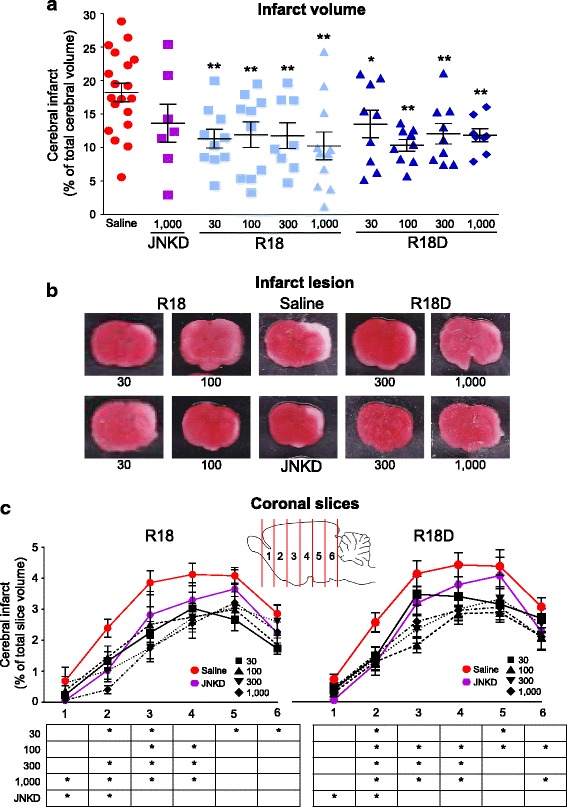
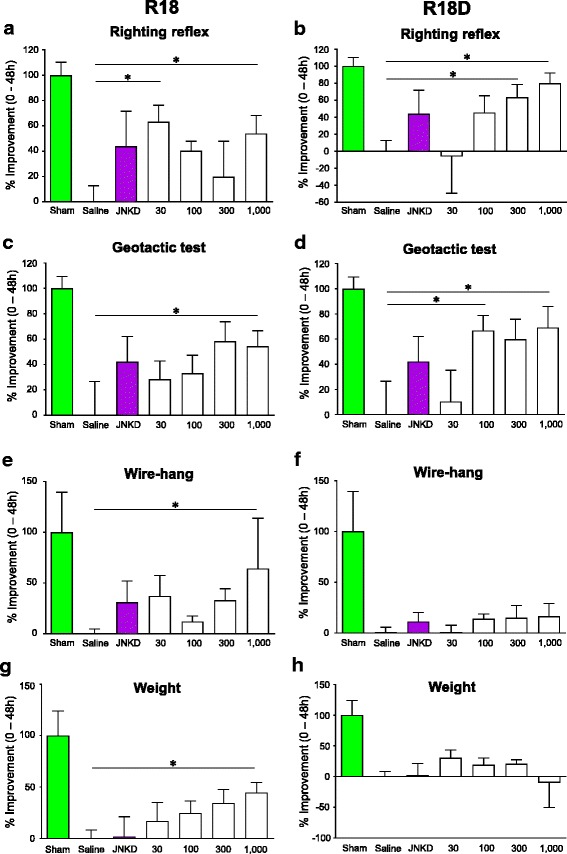
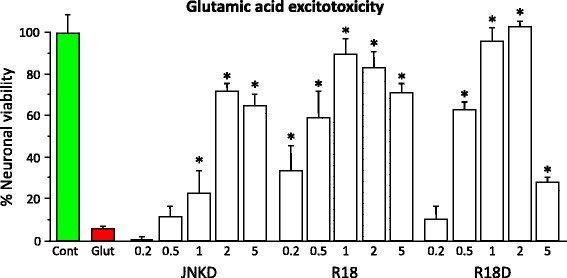
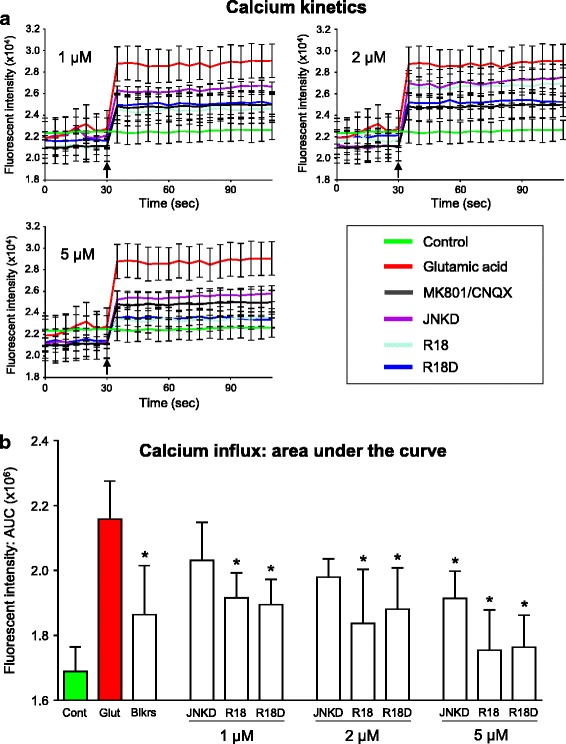
We examined the neuroprotective efficacy of the poly-arginine peptide R18 and its D-enantiomer R18D in a perinatal hypoxic-ischaemic (HI) model in P7 Sprague-Dawley rats. R18 and R18D peptides were administered intraperitoneally at doses of 30, 100, 300 or 1000 nmol/kg immediately after HI (8% O2/92%N2 for 2.5 h). The previously characterised neuroprotective JNKI-1-TATD peptide at a dose of 1000 nmol/kg was used as a control. Infarct volume and behavioural outcomes were measured 48 h after HI. For the R18 and R18D doses examined, total infarct volume was reduced by 25.93% to 43.80% (P = 0.038 to < 0.001). By comparison, the JNKI-1-TATD reduced lesion volume by 25.27% (P = 0.073). Moreover, R18 and R18D treatment resulted in significant improvements in behavioural outcomes, while with JNKI-1-TATD there was a trend towards improvement. As an insight into the likely mechanism underlying the effects of R18, R18D and JNKI-1-TATD, the peptides were added to cortical neuronal cultures exposed to glutamic acid excitotoxicity, resulting in up to 89, 100 and 71% neuroprotection, respectively, and a dose dependent inhibition of neuronal calcium influx. The study further confirms the neuroprotective properties of poly-arginine peptides, and suggests a potential therapeutic role for R18 and R18D in the treatment of HIE.
Keywords: Cationic arginine-rich peptides (CARPs); Hypoxia-ischaemia; Hypoxic-ischaemic encephalopathy; Neuroprotection; Poly-arginine peptides; R18.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
B.P. Meloni and N.W. Knuckey are named inventors of several patent applications regarding the use of arginine-rich peptides as neuroprotective agents. The other authors declare no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
