

Assessment of fluid responsiveness in spontaneously breathing patients: a systematic review of literature
- PMID: 29427013
- PMCID: PMC5807252
- DOI: 10.1186/s13613-018-0365-y
Assessment of fluid responsiveness in spontaneously breathing patients: a systematic review of literature
Abstract
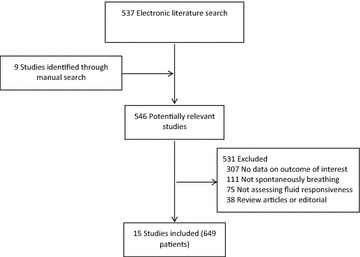
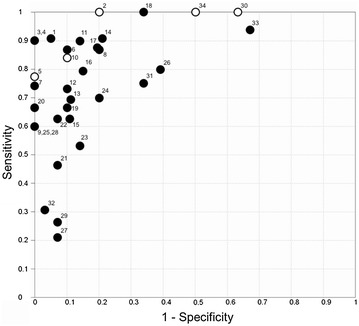
Patients who increase stoke volume or cardiac index more than 10 or 15% after a fluid challenge are usually considered fluid responders. Assessment of fluid responsiveness prior to volume expansion is critical to avoid fluid overload, which has been associated with poor outcomes. Maneuvers to assess fluid responsiveness are well established in mechanically ventilated patients; however, few studies evaluated maneuvers to predict fluid responsiveness in spontaneously breathing patients. Our objective was to perform a systematic review of literature addressing the available methods to assess fluid responsiveness in spontaneously breathing patients. Studies were identified through electronic literature search of PubMed from 01/08/2009 to 01/08/2016 by two independent authors. No restrictions on language were adopted. Quality of included studies was evaluated with Quality Assessment of Diagnostic Accuracy Studies tool. Our search strategy identified 537 studies, and 9 studies were added through manual search. Of those, 15 studies (12 intensive care unit patients; 1 emergency department patients; 1 intensive care unit and emergency department patients; 1 operating room) were included in this analysis. In total, 649 spontaneously breathing patients were assessed for fluid responsiveness. Of those, 340 (52%) were deemed fluid responsive. Pulse pressure variation during the Valsalva maneuver (∆PPV) of 52% (AUC ± SD: 0.98 ± 0.03) and passive leg raising-induced change in stroke volume (∆SV-PLR) > 13% (AUC ± SD: 0.96 ± 0.03) showed the highest accuracy to predict fluid responsiveness in spontaneously breathing patients. Our systematic review indicates that regardless of the limitations of each maneuver, fluid responsiveness can be assessed in spontaneously breathing patients. Further well-designed studies, with adequate simple size and power, are necessary to confirm the real accuracy of the different methods used to assess fluid responsiveness in this population of patients.
Keywords: Critical care; Echocardiography; Fluid responsiveness; Intensive care; Pulse pressure; Spontaneously breathing; Stroke volume.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
