

The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities
- PMID: 29428394
- PMCID: PMC8063758
- DOI: 10.1016/j.neubiorev.2018.02.001
The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities
Abstract
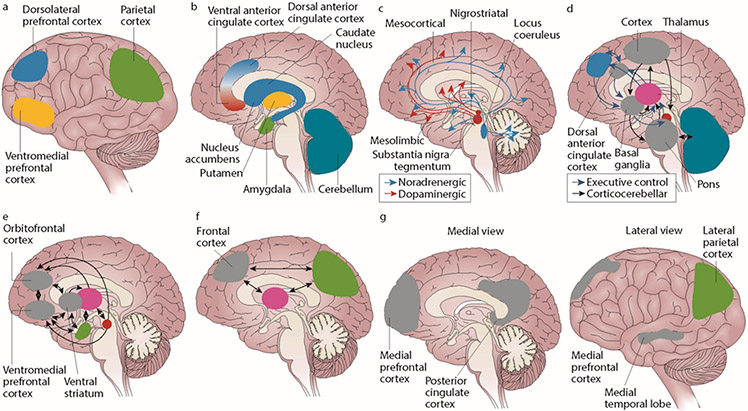
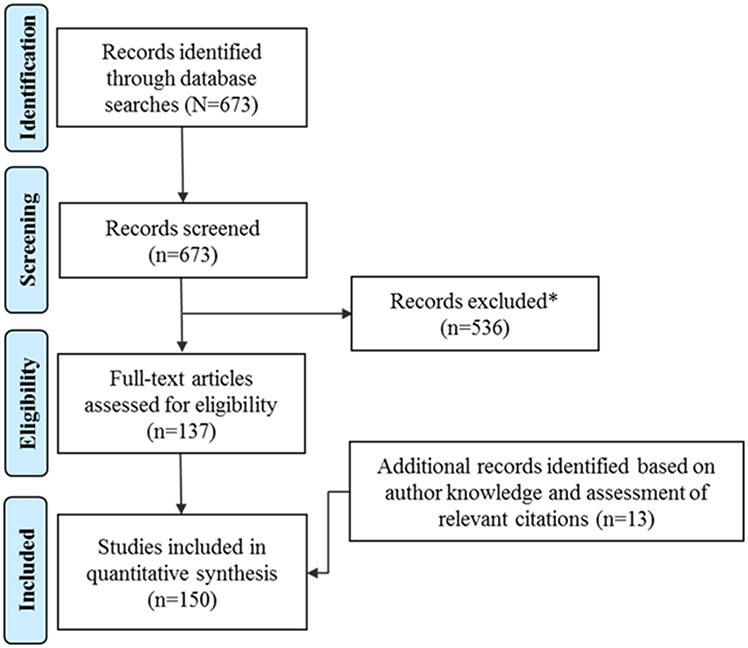
Psychostimulants, including amphetamines and methylphenidate, are first-line pharmacotherapies for individuals with attention-deficit/hyperactivity disorder (ADHD). This review aims to educate physicians regarding differences in pharmacology and mechanisms of action between amphetamine and methylphenidate, thus enhancing physician understanding of psychostimulants and their use in managing individuals with ADHD who may have comorbid psychiatric conditions. A systematic literature review of PubMed was conducted in April 2017, focusing on cellular- and brain system-level effects of amphetamine and methylphenidate. The primary pharmacologic effect of both amphetamine and methylphenidate is to increase central dopamine and norepinephrine activity, which impacts executive and attentional function. Amphetamine actions include dopamine and norepinephrine transporter inhibition, vesicular monoamine transporter 2 (VMAT-2) inhibition, and monoamine oxidase activity inhibition. Methylphenidate actions include dopamine and norepinephrine transporter inhibition, agonist activity at the serotonin type 1A receptor, and redistribution of the VMAT-2. There is also evidence for interactions with glutamate and opioid systems. Clinical implications of these actions in individuals with ADHD with comorbid depression, anxiety, substance use disorder, and sleep disturbances are discussed.
Keywords: Amphetamine; Attention-deficit/hyperactivity disorder; Methylphenidate; Pharmacology.
Copyright © 2018 The Author. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Lahey BB, Applegate B, McBurnett K, Biederman J, Greenhill L, Hynd GW, et al. DSM-IV field trials for attention deficit hyperactivity disorder in children and adolescents. Am J Psychiatry. 1994;151(11):1673–85. - PubMed
-
- Barkley RA, Fischer M, Smallish L, Fletcher K. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. J Abnorm Psychol. 2002;111(2):279–89. - PubMed
-
- Weiss G, Hechtman L, Milroy T, Perlman T. Psychiatric status of hyperactives as adults: a controlled prospective 15-year follow-up of 63 hyperactive children. J Am Acad Child Psychiatry. 1985;24(2):211–20. - PubMed
-
- Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159–65. - PubMed
-
- Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
