

Impact of Body Mass Index on Heart Failure by Race/Ethnicity From the Get With The Guidelines-Heart Failure (GWTG-HF) Registry
- PMID: 29428434
- PMCID: PMC5834392
- DOI: 10.1016/j.jchf.2017.11.011
Impact of Body Mass Index on Heart Failure by Race/Ethnicity From the Get With The Guidelines-Heart Failure (GWTG-HF) Registry
Abstract
Objectives: This study sought to evaluate the influence of race/ethnicity on the relationship between body mass index (BMI) and mortality in heart failure with preserved ejection fraction (HFpEF) and HF with reduced EF (HFrEF) patients.
Background: Prior studies demonstrated an "obesity paradox" among overweight and obese patients, where they have a better HF prognosis than normal weight patients. Less is known about the relationship between BMI and mortality among diverse patients with HF, particularly given disparities in obesity and HF prevalence.
Methods: The authors used Get With The Guidelines-Heart Failure data to assess the relationship between BMI and in-hospital mortality by using logistic regression modeling. The authors assessed 30-day and 1-year rates of all-cause mortality following discharge by using Cox regression modeling.
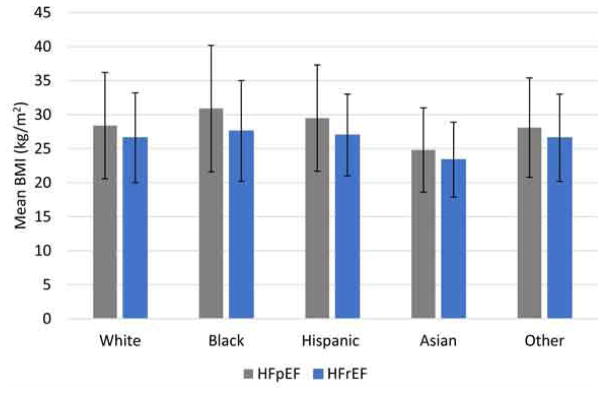
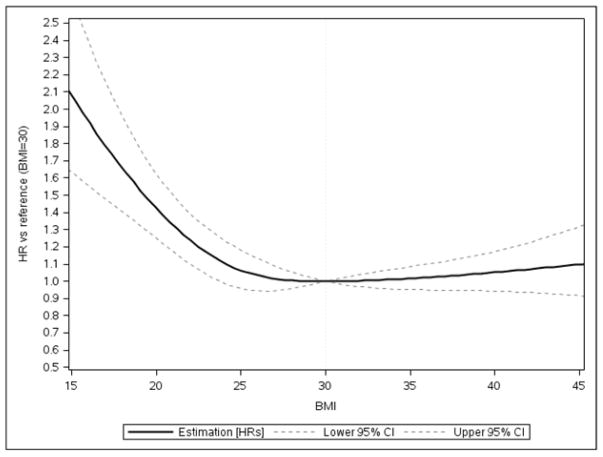
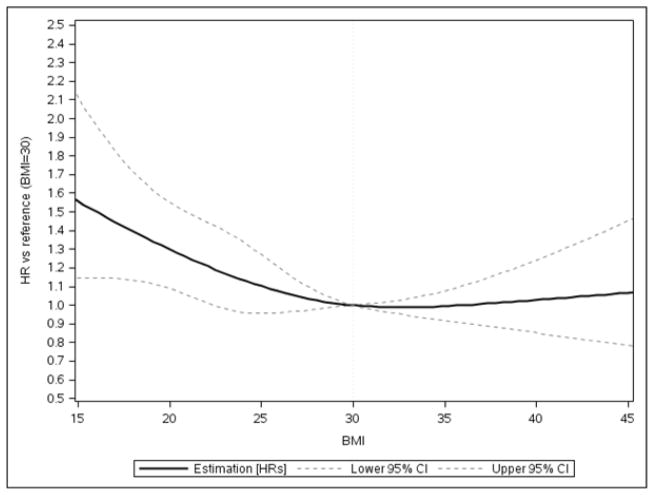
Results: A total of 39,647 patients with HF were included (32,434 [81.8%] white subjects; 3,809 [9.6%] black subjects; 1,928 [4.9%] Hispanic subjects; 544 [1.4%] Asian subjects; and 932 [2.3%] other subjects); 59.7% of subjects had HFpEF, and 30.7% were obese. More black and Hispanic patients had Class I or higher obesity (BMI ≥30 kg/m2) than whites, Asians, or other racial/ethnic groups (p < 0.0001). Among subjects with HFpEF, higher BMI was associated with lower 30-day mortality, up to 30 kg/m2 with a small risk increase above 30 kg/m2 (BMI: 30 vs. 18.5 kg/m2), hazard ratio (HR) of 0.63 (95% confidence interval [CI]: 0.54 to 0.73). A modest relationship was observed in HFrEF subjects (BMI: 30 vs. 18.5 kg/m2; HR: 0.73; 95% CI: 0.60 to 0.89), with no risk increase above 30 kg/m2. There were no significant interactions between BMI and race or ethnicity related to 30-day mortality (p > 0.05).
Conclusions: This work is one of the first suggesting the obesity paradox for 30-day mortality exists at all BMI levels in HFrEF but not in patients with HFpEF. Higher BMI was associated with lower 30-day mortality across racial/ethnic groups in a manner inconsistent with the J-shaped relationship noted for coronary artery disease. The differential slope of obesity and mortality among HFpEF and patients with HFrEF potentially suggests differing mechanistic factors, requiring further exploration.
Keywords: GWTG-Heart Failure; ethnicity; heart failure; mortality; obesity; race.
Published by Elsevier Inc.
Figures

Comment in
-
Body Mass Index and Heart Failure Mortality: More Is Less?JACC Heart Fail. 2018 Mar;6(3):243-245. doi: 10.1016/j.jchf.2017.12.013. Epub 2018 Feb 7. JACC Heart Fail. 2018. PMID: 29428435 Free PMC article. No abstract available.
References
-
- Mandviwala T, Khalid U, Deswal A. Obesity and Cardiovascular Disease: a Risk Factor or a Risk Marker? Curr Atheroscler Rep. 2016;18:21. - PubMed
-
- Department of Health and Human Services, Centers for Disease Control and Prevention. Heart Failure Fact Sheet. 2016 https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/docs/fs_heart_fail....
-
- Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff (Millwood) 2009;28:w822–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
