

Advances in Tissue Engineering Techniques for Articular Cartilage Repair
- PMID: 29430164
- PMCID: PMC5805482
- DOI: 10.1053/j.oto.2009.10.004
Advances in Tissue Engineering Techniques for Articular Cartilage Repair
Abstract
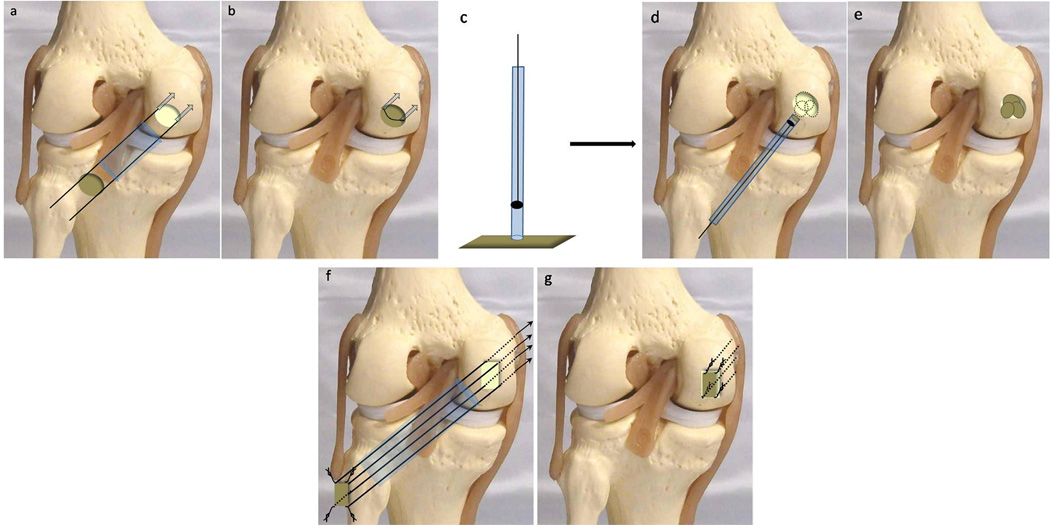
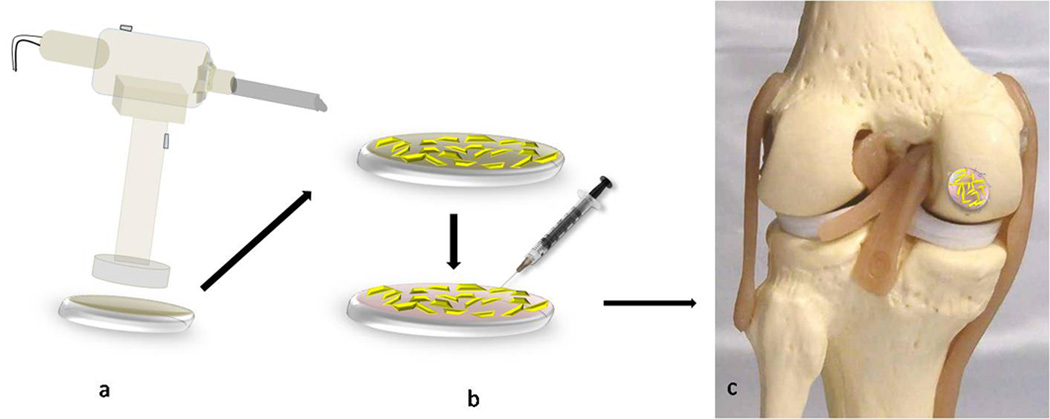
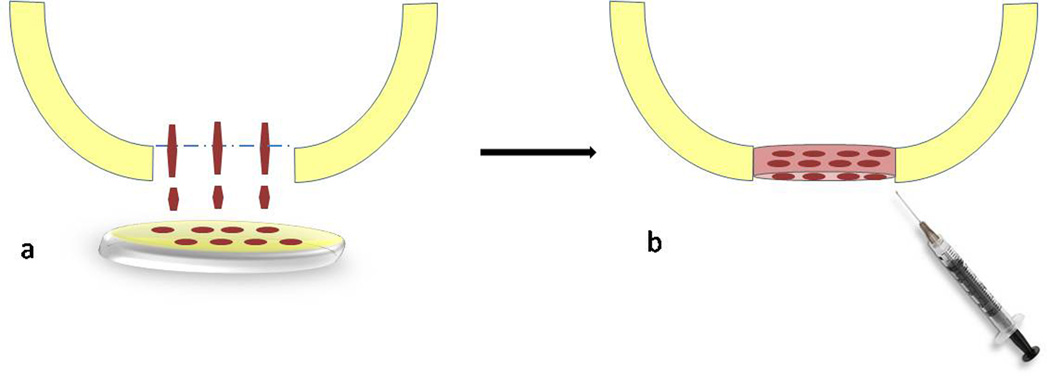
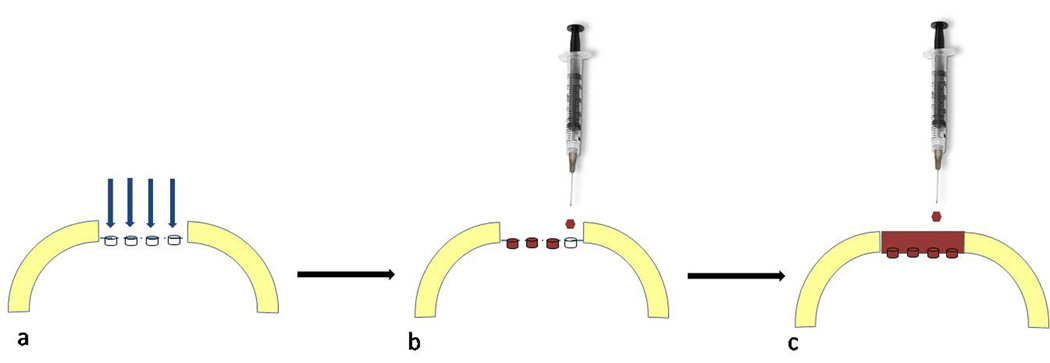
The limited repair potential of human articular cartilage contributes to development of debilitating osteoarthritis and remains a great clinical challenge. This has led to evolution of cartilage treatment strategies from palliative to either reconstructive or reparative methods in an attempt to delay or "bridge the gap" to joint replacement. Further development of tissue engineering-based cartilage repair methods have been pursued to provide a more functional biological tissue. Currently, tissue engineering of articular cartilage has three cornerstones; a cell population capable of proliferation and differentiation into mature chondrocytes, a scaffold that can host these cells, provide a suitable environment for cellular functioning and serve as a sustained-release delivery vehicle of chondrogenic growth factors and thirdly, signaling molecules and growth factors that stimulate the cellular response and the production of a hyaline extracellular matrix (ECM). The aim of this review is to summarize advances in each of these three fields of tissue engineering with specific relevance to surgical techniques and technical notes.
Figures

References
-
- Chu CR, Convery FR, Akeson WH, Meyers M, Amiel D. Articular cartilage transplantation. Clinical results in the knee. Clin Orthop Relat Res. 1999 Mar;360:159–168. - PubMed
-
- Brittberg M, Lindahl A, Nilsson A, et al. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med. 1994;331:889–895. - PubMed
-
- Saris DB, Vanlauwe J, Victor J, Haspl M, Bohnsack M, Fortems Y, Vandekerckhove B, Almqvist KF, Claes T, Handelberg F, Lagae K, van der Bauwhede J, Vandenneucker H, Yang KG, Jelic M, Verdonk R, Veulemans N, Bellemans J, Luyten FP. Characterized chondrocyte implantation results in better structural repair when treating symptomatic cartilage defects of the knee in a randomized controlled trial versus microfracture. Am J Sports Med. 2008 Feb;36(2):235–246. - PubMed
-
- Salgado AJ, Oliveira JT, Pedro AJ, Reis RL. Adult stem cells in bone and cartilage tissue engineering. Curr Stem Cell Res Ther. 2006;1:345–364. - PubMed
-
- Kisiday JD, Kopesky PW, Evans CH, Grodzinsky AJ, McIlwraith CW, Frisbie DD. Evaluation of adult equine bone marrow- and adipose-derived progenitor cell chondrogenesis in hydrogel cultures. J Orthop Res. 2008;26:322–331. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous