

Acute kidney injury and infections in patients taking antihypertensive drugs: a self-controlled case series analysis
- PMID: 29430198
- PMCID: PMC5796801
- DOI: 10.2147/CLEP.S146757
Acute kidney injury and infections in patients taking antihypertensive drugs: a self-controlled case series analysis
Abstract
Background: The relative risk of acute kidney injury (AKI) following different infections, and whether angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs) modify the risk, is unclear. We aimed to determine the risks of hospital admission with AKI following infections (urinary tract infection [UTI], lower respiratory tract infection [LRTI], and gastroenteritis) among users of antihypertensive drugs.
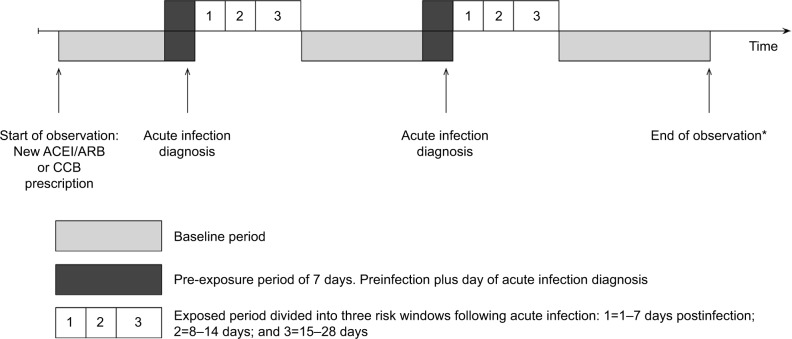
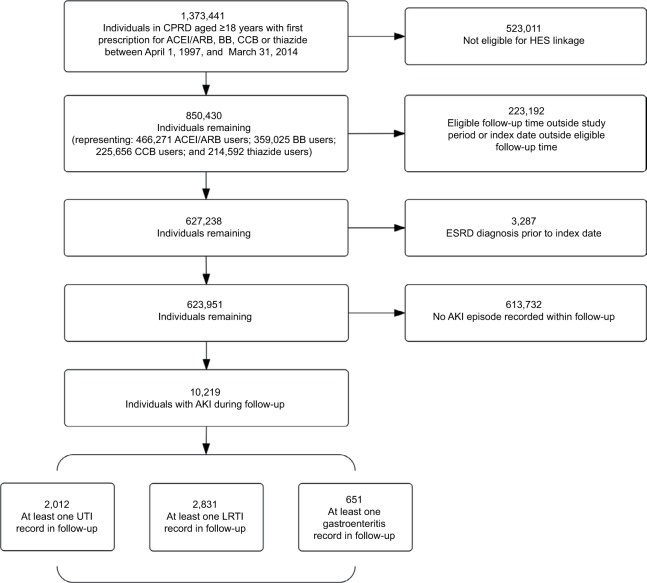
Methods: We used UK electronic health records from practices contributing to the Clinical Practice Research Datalink linked to the Hospital Episode Statistics database. We identified adults initiating ACEIs/ARBs or alternative antihypertensive therapy (β-blockers, calcium channel blockers, or thiazide diuretics) between April 1997 and March 2014 with at least 1 year of primary care registration prior to first prescription, who had a hospital admission for AKI, and who had a primary care record for incident UTI, LRTI, or gastroenteritis. We used a self-controlled case series design to calculate age-adjusted incidence rate ratios (IRRs) for AKI during risk periods following acute infection relative to noninfected periods (baseline).
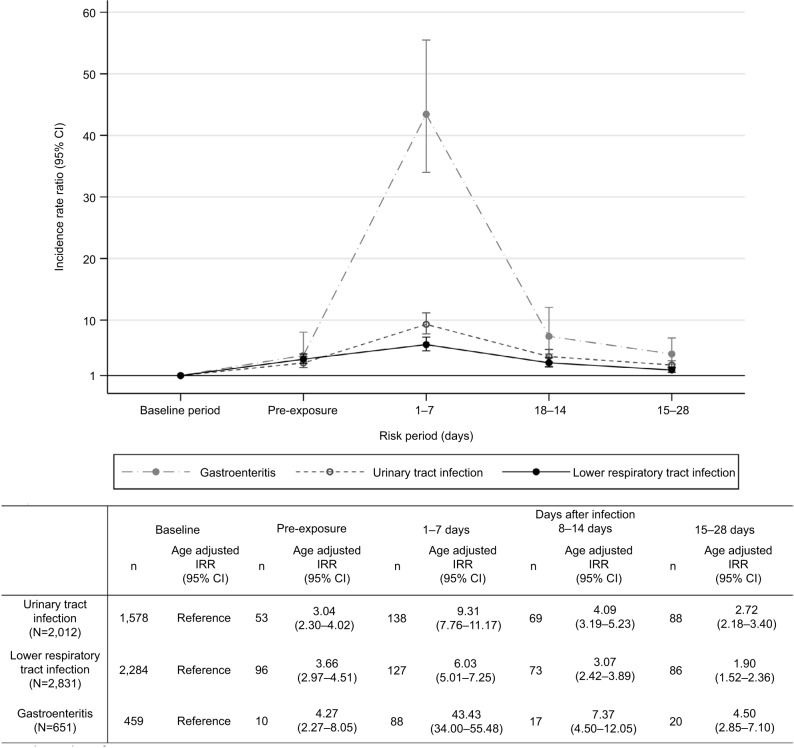
Results: We identified 10,219 eligible new users of ACEIs/ARBs or other antihypertensives with an AKI record. Among these, 2,012 had at least one record for a UTI during follow-up, 2,831 had a record for LRTI, and 651 had a record for gastroenteritis. AKI risk was higher following infection than in baseline noninfectious periods. The rate ratio was highest following gastroenteritis: for the period 1-7 days postinfection, the IRR for AKI following gastroenteritis was 43.4 (95% CI=34.0-55.5), compared with 6.0 following LRTI (95% CI=5.0-7.3), and 9.3 following UTI (95% CI=7.8-11.2). Increased risks were similar for different antihypertensives.
Conclusion: Acute infections are associated with substantially increased transient AKI risk among antihypertensive users, with the highest risk after gastroenteritis. The increase in relative risk is not greater among users of ACEIs/ARBs compared with users of other antihypertensives.
Keywords: acute kidney injury; angiotensin receptor antagonists; angiotensin-converting enzyme inhibitors; infection; self-controlled case series.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365–3370. - PubMed
-
- Kerr M, Bedford M, Matthews B, O’Donoghue D. The economic impact of acute kidney injury in England. Nephrol Dial Transplant. 2014;29(7):1362–1368. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
