

Electrical impedance tomography
- PMID: 29430443
- PMCID: PMC5799136
- DOI: 10.21037/atm.2017.12.06
Electrical impedance tomography
Abstract
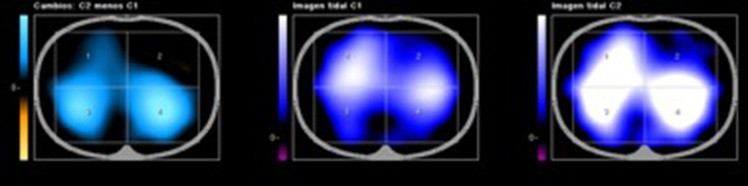
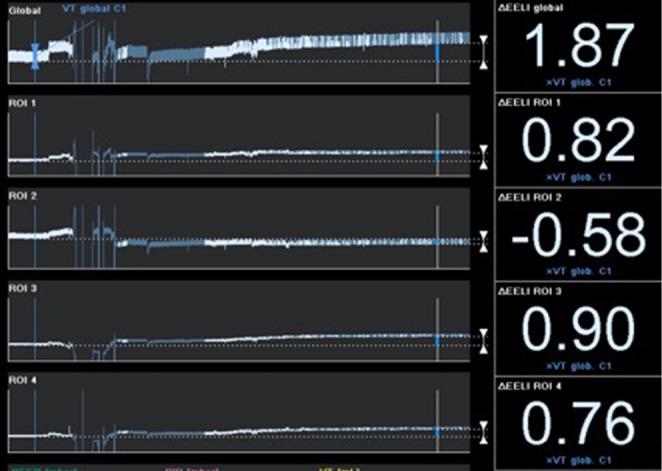
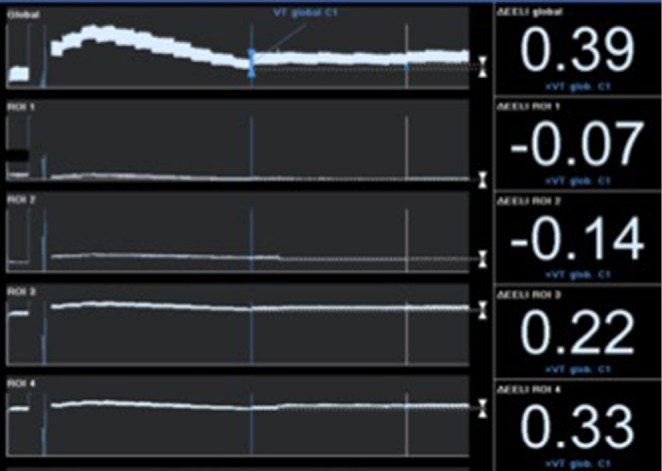
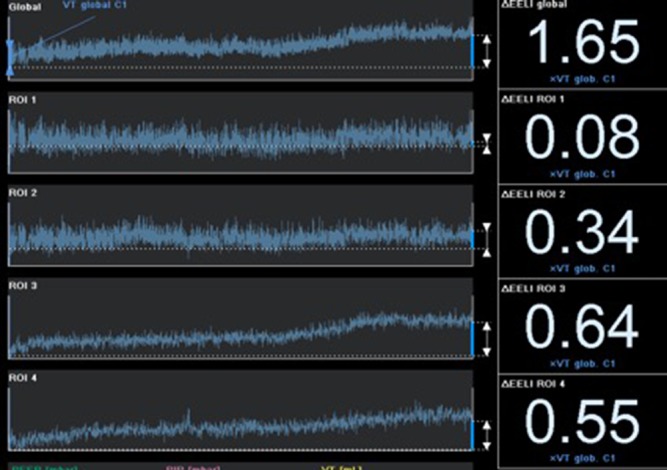
Continuous assessment of respiratory status is one of the cornerstones of modern intensive care unit (ICU) monitoring systems. Electrical impedance tomography (EIT), although with some constraints, may play the lead as a new diagnostic and guiding tool for an adequate optimization of mechanical ventilation in critically ill patients. EIT may assist in defining mechanical ventilation settings, assess distribution of tidal volume and of end-expiratory lung volume (EELV) and contribute to titrate positive end-expiratory pressure (PEEP)/tidal volume combinations. It may also quantify gains (recruitment) and losses (overdistention or derecruitment), granting a more realistic evaluation of different ventilator modes or recruitment maneuvers, and helping in the identification of responders and non-responders to such maneuvers. Moreover, EIT also contributes to the management of life-threatening lung diseases such as pneumothorax, and aids in guiding fluid management in the critical care setting. Lastly, assessment of cardiac function and lung perfusion through electrical impedance is on the way.
Keywords: Acute lung injury; critical care; electric impedance; physiologic monitoring; respiratory distress syndrome.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical