

Combined BRAF, EGFR, and MEK Inhibition in Patients with BRAFV600E-Mutant Colorectal Cancer
- PMID: 29431699
- PMCID: PMC5882509
- DOI: 10.1158/2159-8290.CD-17-1226
Combined BRAF, EGFR, and MEK Inhibition in Patients with BRAFV600E-Mutant Colorectal Cancer
Abstract
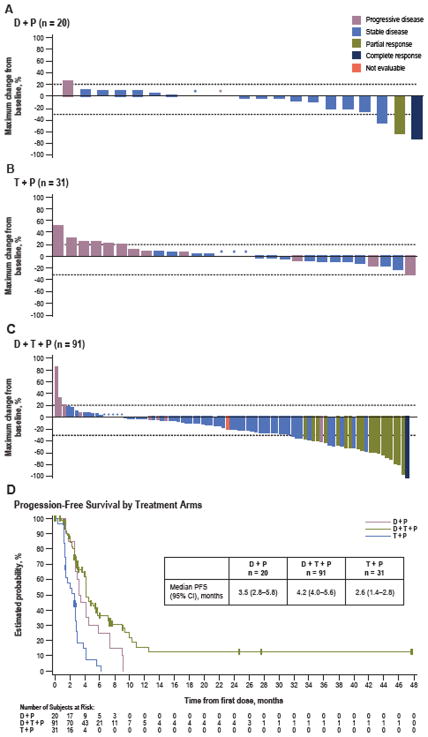
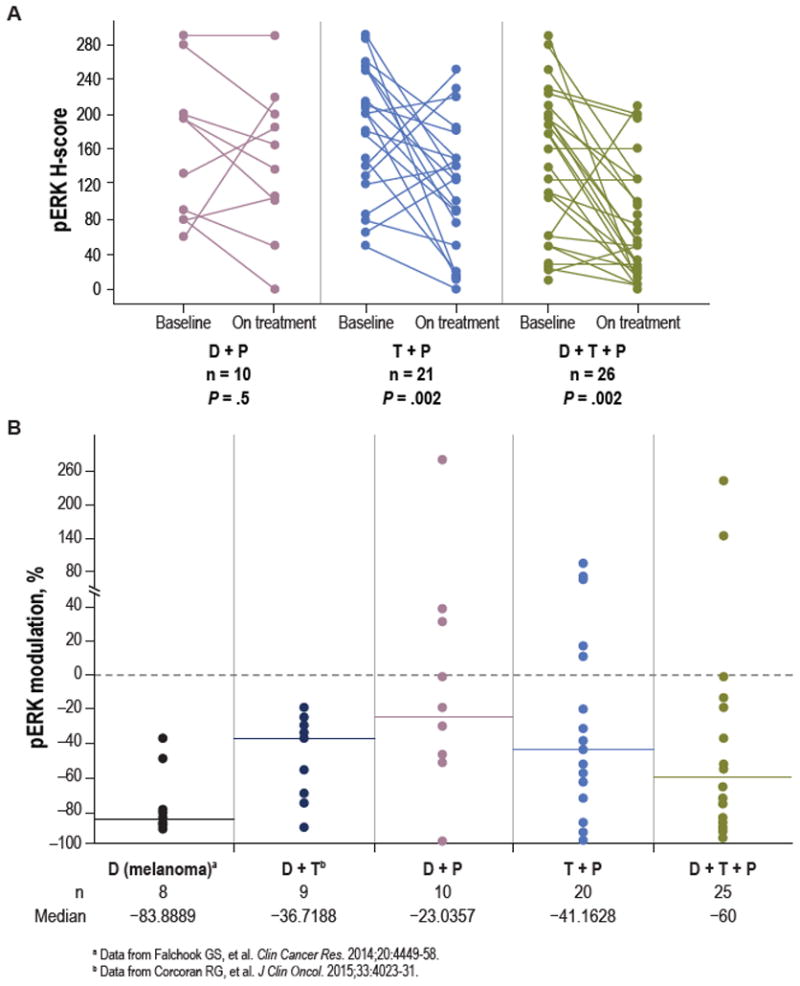
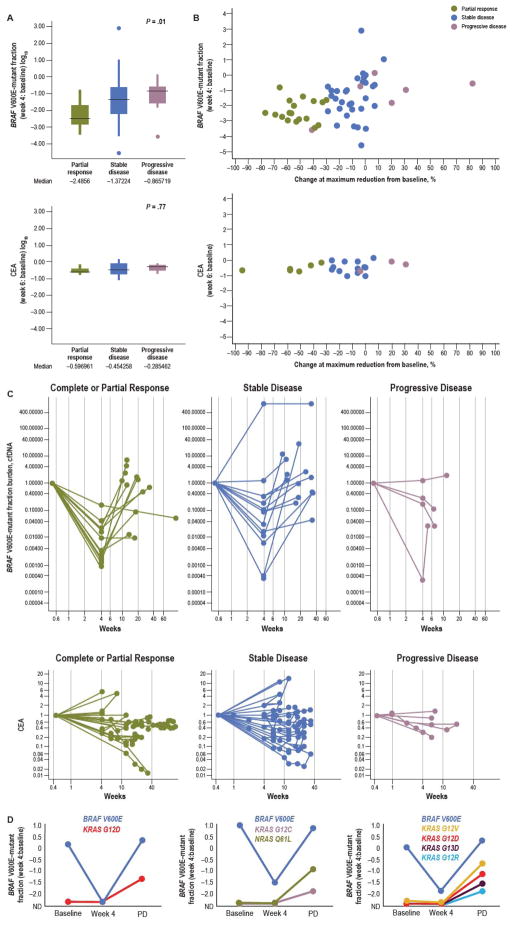
Although BRAF inhibitor monotherapy yields response rates >50% in BRAFV600-mutant melanoma, only approximately 5% of patients with BRAFV600E colorectal cancer respond. Preclinical studies suggest that the lack of efficacy in BRAFV600E colorectal cancer is due to adaptive feedback reactivation of MAPK signaling, often mediated by EGFR. This clinical trial evaluated BRAF and EGFR inhibition with dabrafenib (D) + panitumumab (P) ± MEK inhibition with trametinib (T) to achieve greater MAPK suppression and improved efficacy in 142 patients with BRAFV600E colorectal cancer. Confirmed response rates for D+P, D+T+P, and T+P were 10%, 21%, and 0%, respectively. Pharmacodynamic analysis of paired pretreatment and on-treatment biopsies found that efficacy of D+T+P correlated with increased MAPK suppression. Serial cell-free DNA analysis revealed additional correlates of response and emergence of KRAS and NRAS mutations on disease progression. Thus, targeting adaptive feedback pathways in BRAFV600E colorectal cancer can improve efficacy, but MAPK reactivation remains an important primary and acquired resistance mechanism.Significance: This trial demonstrates that combined BRAF + EGFR + MEK inhibition is tolerable, with promising activity in patients with BRAFV600E colorectal cancer. Our findings highlight the MAPK pathway as a critical target in BRAFV600E colorectal cancer and the need to optimize strategies inhibiting this pathway to overcome both primary and acquired resistance. Cancer Discov; 8(4); 428-43. ©2018 AACR.See related commentary by Janku, p. 389See related article by Hazar-Rethinam et al., p. 417This article is highlighted in the In This Issue feature, p. 371.
©2018 American Association for Cancer Research.
Conflict of interest statement
R.B. Corcoran is a consultant/advisory board member for Amgen, Astex Pharmaceuticals, Avidity Biosciences, BMS, Genentech, Merrimack, N-of-one, Roche, Shire, and Taiho and has received research funding from AstraZeneca and Sanofi.
T. André reports a scientific advisory role/consultant for Amgen, Bristol-Myers Squibb, MSD Oncology, Sanofi, Servier, Roche and Xbiotech and has received honoraria from Amgen, BMS, Bayer, Baxter, Celgene, Lilly, Novartis, Roche, and Yakult.
C. Atreya reports reseach grants from GlaxoSmithKline, Merck, and Novartis and is a consultant/advisory board member of Bayer Diagnostics and Genentech.
J.H.M. Schellens reported an advisory role for AstraZeneca, Sotio, Roche, Merck and MerckSerono and stock in Modra Pharmaceuticals bv.
T. Yoshino reports a research grant from GlaxoSmithKline K.K. and a grant from Boehringer Ingelheim GmbH outside the submitted work.
Y. Humblet has been invited by Merck KGaA and Sanofi to international oncology meetings, and his hospital has received money for patient follow-up compensation.
A.J. McRee is an advisory board member for Merck.
S. Siena reports a scientific advisory role for Amgen, Bayer, Eli Lilly, Ignyta, Merck, Novartis, Roche, and Sanofi.
G. Middleton reports research grants from AstraZeneca, GemVax & Kael, and Merck, Sharpe, and Dohme, reports equity ownership in PhosImmune, and has received honoraria from BMS and Eli Lilly.
K. Muro reports receipt of honoraria from Chugai, Merck Serono, Taiho, Takeda, and Yakult, and reports a scientific advisory role for Eli Lilly and Ono.
M.S. Gordon reports consultancy, involvement in speakers bureau, and a scientific advisory role for, equity ownership in, and research funding support, honoraria, and patents and royalties from, GlaxoSmithKline.
J. Tabernero reports a scientific advisory role for Amgen, Bayer, Boehringer Ingelheim, Celgene, Chugai, Genentech, Inc., Lilly, MSD, Merck Serono, Novartis, Pfizer, F. Hoffmann-La Roche Ltd, Sanofi, Symphogen, Taiho, and Takeda.
R. Yaeger reports consulting or advisory roles for Advaxis and GlaxoSmithKline.
P. J. O’Dwyer has received consulting fees from Genentech, BMS, Boehringer Ingelheim, and clinical trials support from Genentech, BMS, AZ, Celgene, Merck, Syndax, GSK, Abbvie, Incyte, Minneamrata, Pharmacyclics, Five Prime, and Fortyseven.
A.S. Jung is an employee of and owns stock in Amgen.
J.C. Brase is an employee of Novartis.
S Jaeger was an employee of Novartis during the conduct of this study and writing of the report.
S. Bettinger is an employee of Novartis.
B Mookerjee is an employee of Novartis and owns stock in GlaxoSmithKline and Novartis.
F. Rangwala is an employee of Novartis.
E.Van Cutsem reports consulting or advisory roles for Bayer, Lilly, Roche, and Servier and has received research funding from Amgen, Bayer, Boehringer Ingelheim, Lilly, Novartis, Roche, Sanofi, Celgene, Ipsen, Merck, Merck KGaA, and Servier.
The remaining authors declare no potential conflicts of interest.
Figures

Comment in
-
Advances on the BRAF Front in Colorectal Cancer.Cancer Discov. 2018 Apr;8(4):389-391. doi: 10.1158/2159-8290.CD-18-0125. Cancer Discov. 2018. PMID: 29610287
References
-
- Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417(6892):949–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
