

Hepatitis B/C in the countries of the EU/EEA: a systematic review of the prevalence among at-risk groups
- PMID: 29433454
- PMCID: PMC5809955
- DOI: 10.1186/s12879-018-2988-x
Hepatitis B/C in the countries of the EU/EEA: a systematic review of the prevalence among at-risk groups
Abstract
Background: In 2016, the World Health Organisation set a goal to eliminate viral hepatitis by 2030. Robust epidemiological information underpins all efforts to achieve elimination and this systematic review provides estimates of HBsAg and anti-HCV prevalence in the European Union/European Economic Area (EU/EEA) among three at-risk populations: people in prison, men who have sex with men (MSM), and people who inject drugs (PWID).
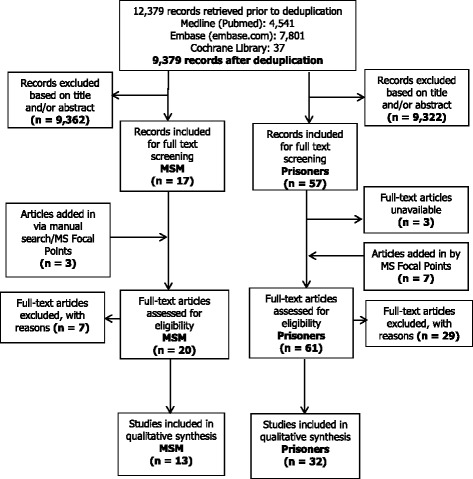
Methods: Estimates of the prevalence among the three risk groups included in our study were derived from multiple sources. A systematic search of literature published during 2005-2015 was conducted without linguistic restrictions to identify studies among people in prison and HIV negative/HIV sero-status unknown MSM. National surveillance focal points were contacted to validate the search results. Studies were assessed for risk of bias and high quality estimates were pooled at country level. PWID data were extracted from the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) repository.
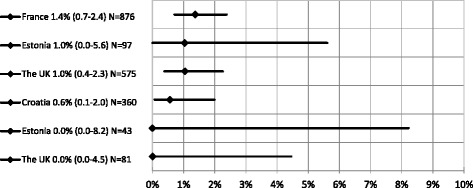
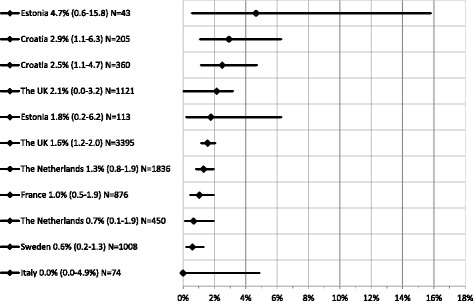
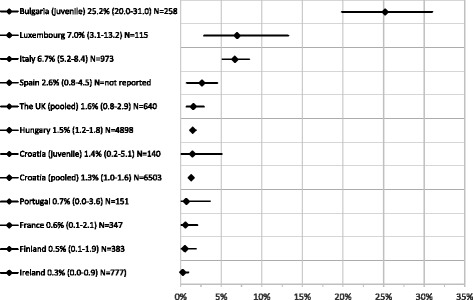
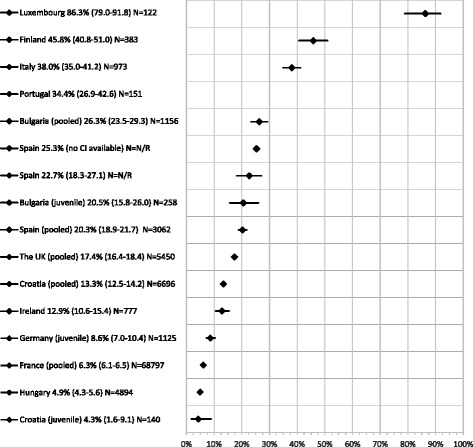
Results: Despite gaps, we report 68 single study/pooled HBsAg/anti-HCV prevalence estimates covering 23/31 EU/EEA countries, 42 of which were of intermediate/high prevalence using the WHO endemicity threshold (of ≥2%). This includes 20 of the 23 estimates among PWID, 20 of the 28 high quality estimates among people in prison, and four of the 17 estimates among MSM. In general terms, the highest HBsAg prevalence was found among people in prison (range of 0.3% - 25.2%) followed by PWID (0.5% - 6.1%) and MSM (0.0% - 1.4%). The highest prevalence of anti-HCV was also found among people in prison (4.3% - 86.3%) and PWID (13.8% - 84.3%) followed by MSM (0.0% - 4.7%).
Conclusions: Our results suggest prioritisation of PWID and the prison population as the key populations for HBV/HCV screening and treatment given their dynamic interaction and high prevalence. The findings of this study do not seem to strongly support the continued classification of MSM as a high risk group for chronic hepatitis B infection. However, we still consider MSM a key population for targeted action given the emerging evidence of viral hepatitis transmission within this risk group together with the complex interaction of HBV/HCV and HIV.
Keywords: Hepatitis B; Hepatitis C; Higher risk groups; Men who have sex with men; People who inject drugs; Prevalence; Prisoners; Systematic review [publication type].
Conflict of interest statement
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Control ECfDPa. Annual epidemiological report for 2015 – hepatitis B. Stockholm: 2015.
-
- European Centre for Disease Prevention and Control (ECDC). Annual Epidemiological Report for 2015 - Hepatitis C. Stockholm: 2015.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
