

Tinnitus services in the United Kingdom: a survey of patient experiences
- PMID: 29433479
- PMCID: PMC5809968
- DOI: 10.1186/s12913-018-2914-3
Tinnitus services in the United Kingdom: a survey of patient experiences
Abstract
Background: Tinnitus service provision in the United Kingdom has been investigated from the healthcare provider's perspective demonstrating considerable regional variation particularly regarding availability of psychological treatments. An audiological-based tinnitus service, however, was reportedly available for all tinnitus patients in the UK. The aim of the current study was to define and evaluate nationwide tinnitus healthcare services from the patients' viewpoint.
Methods: Secondary analyses were performed on data from a 33-item questionnaire provided by the British Tinnitus Association. The questionnaire had been distributed via email and social media.
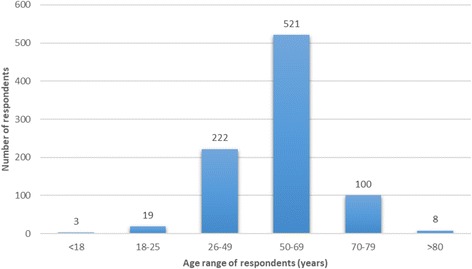
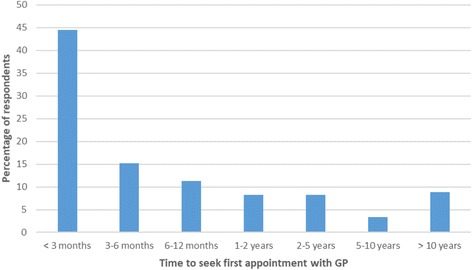
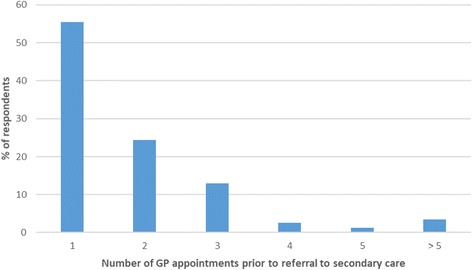
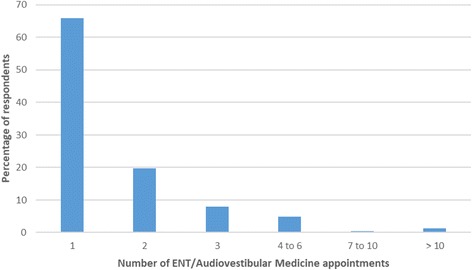
Results: Responses from 937 participants who had or had previously experienced tinnitus were analysed. All but one person had at some time consulted their GP. About one in five received medication in primary care. The majority were referred to secondary care, generally an ENT surgeon or audiovestibular physician; some were referred directly to audiological services. In secondary care the majority underwent audiometric testing and over half underwent MRI scanning. Drugs were prescribed less frequently in secondary care. About one third of patients were referred onwards from diagnostic services in secondary care to receive therapeutic interventions for tinnitus. Therapy was generally delivered by an audiologist or hearing therapist. Just under two fifths of people discharged from secondary care returned to their GP, with most returning within one year. Over a third of this group were re-referred to secondary care. Few patients saw a psychologist (2.6%) though some psychological treatments were delivered by appropriately trained audiologists. Negative counselling from healthcare professionals in both primary and secondary care settings was reported.
Conclusions: Although the UK has developed a national service for patients with tinnitus many people find it difficult to access, being blocked at the primary care level or after secondary care diagnostic services. Many of those discharged from secondary care return to their GP within a short space of time and are re-referred to secondary care creating an unsatisfactory and expensive revolving-door pattern of healthcare. Despite psychological treatment modalities having the best evidence base for successful tinnitus management, only a minority of tinnitus patients ever get to meet a psychologist.
Keywords: Audiology; Primary care; Psychology; Revolving door; Secondary care; Tinnitus.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable: as this study was a retrospective service evaluation and used only highly anonymised data for the sole purpose of service evaluation, individual consent was not sought, and research ethics committee review was not required [19].
Consent for publication
Not applicable.
Competing interests
DM has paid consultancies with Otonomy and has received payment for trials of drugs for tinnitus (GSK and Autifony) and has received payment for providing tinnitus talks to healthcare professionals and the public. DM has received royalties for books on tinnitus. JR has received payment for trials of drugs for tinnitus (Otonomy and Autifony). DS is Chief Executive of a tinnitus charity (British Tinnitus Association). DJH is funded by the NIHR Biomedical Research Centre Programme. The views expressed in this article are those of the authors and not necessarily those of the NIHR, the NHS, or the Department of Health.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Davis A, El Rafaie A. Epidemiology of tinnitus. In: Tyler RS, editor. Tinnitus handbook. San Diego: Singular, Thomson Learning; 2000. pp. 1–23.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
