

Effect of socioeconomic inequalities on cholecystectomy outcomes: a 10-year population-based analysis
- PMID: 29433528
- PMCID: PMC5809951
- DOI: 10.1186/s12939-018-0739-7
Effect of socioeconomic inequalities on cholecystectomy outcomes: a 10-year population-based analysis
Abstract
Background: Although numerous epidemiological studies on cholecystectomy have been conducted worldwide, only a few have considered the effect of socioeconomic inequalities on cholecystectomy outcomes. Specifically, few studies have focused on the low-income population (LIP).
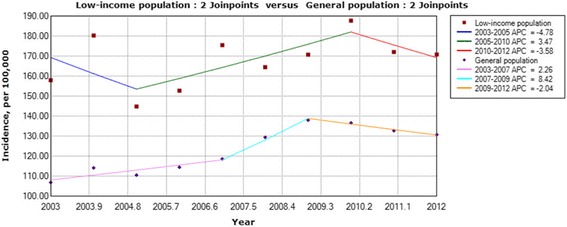
Methods: A nationwide prospective study based on the Taiwan National Health Insurance dataset was conducted during 2003-2012. The International Classification of ICD-9-CM procedure codes 51.2 and 51.21-51.24 were identified as the inclusion criteria for cholecystectomy. Temporal trends were analyzed using a joinpoint regression, and the hierarchical linear modeling (HLM) method was used as an analytical strategy to evaluate the group-level and individual-level factors. Interactions between age, gender and SES were also tested in HLM model.
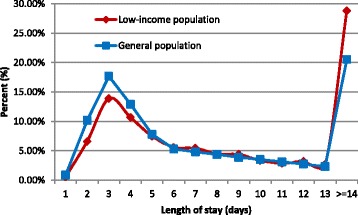
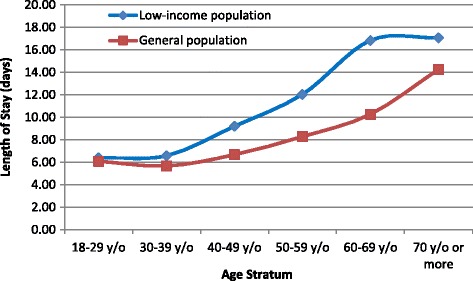
Results: Analyses were conducted on 225,558 patients. The incidence rates were 167.81 (95% CI: 159.78-175.83) per 100,000 individuals per year for the LIP and 123.24 (95% CI: 116.37-130.12) per 100,000 individuals per year for the general population (GP). After cholecystectomy, LIP patients showed higher rates of 30-day mortality, in-hospital complications, and readmission for complications, but a lower rate of routine discharge than GP patients. The hospital costs and length of stay for LIP patients were higher than those for GP patients. The multilevel analysis using HLM revealed that adverse socioeconomic status significantly negatively affects the outcomes of patients undergoing cholecystectomy. Additionally, male sex, advanced age, and high Charlson Comorbidity Index (CCI) scores were associated with higher rates of in-hospital complications and 30-day mortality. We also observed that the 30-day mortality rates for patients who underwent cholecystectomy in regional hospitals and district hospitals were significantly higher than those of patients receiving care in a medical center.
Conclusion: Patients with a disadvantaged finance status appeared to be more vulnerable to cholecystectomy surgery. This result suggested that further interventions in the health care system are necessary to reduce this disparity.
Keywords: Acute cholecystitis; Cholecystectomy; Gallbladder disease; Socioeconomic status.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the research ethics committee of the Taoyuan General Hospital (Approval Number: TYGH103015), which has been certified by the Ministry of Health & Welfare of Taiwan, and the research protocol was reviewed by the National Health Research Institutes (Agreement Number: NHIRD-104-081).
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no conflicts of interest, including directorships, stock holdings or contracts.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Edwards HC. Diseases of the gallbladder. Berlin Heidelberg: Springer; 2000.
-
- Phatak UR, Albarado R, Eachempati SR. Management of Cholecystitis in high-risk patients. Springer Int Publ. 2015;
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
