

Association between clinicopathological factors and postoperative radiotherapy in patients with completely resected pathological N2 non-small cell lung cancer
- PMID: 29434986
- PMCID: PMC5777368
- DOI: 10.3892/ol.2017.7601
Association between clinicopathological factors and postoperative radiotherapy in patients with completely resected pathological N2 non-small cell lung cancer
Abstract
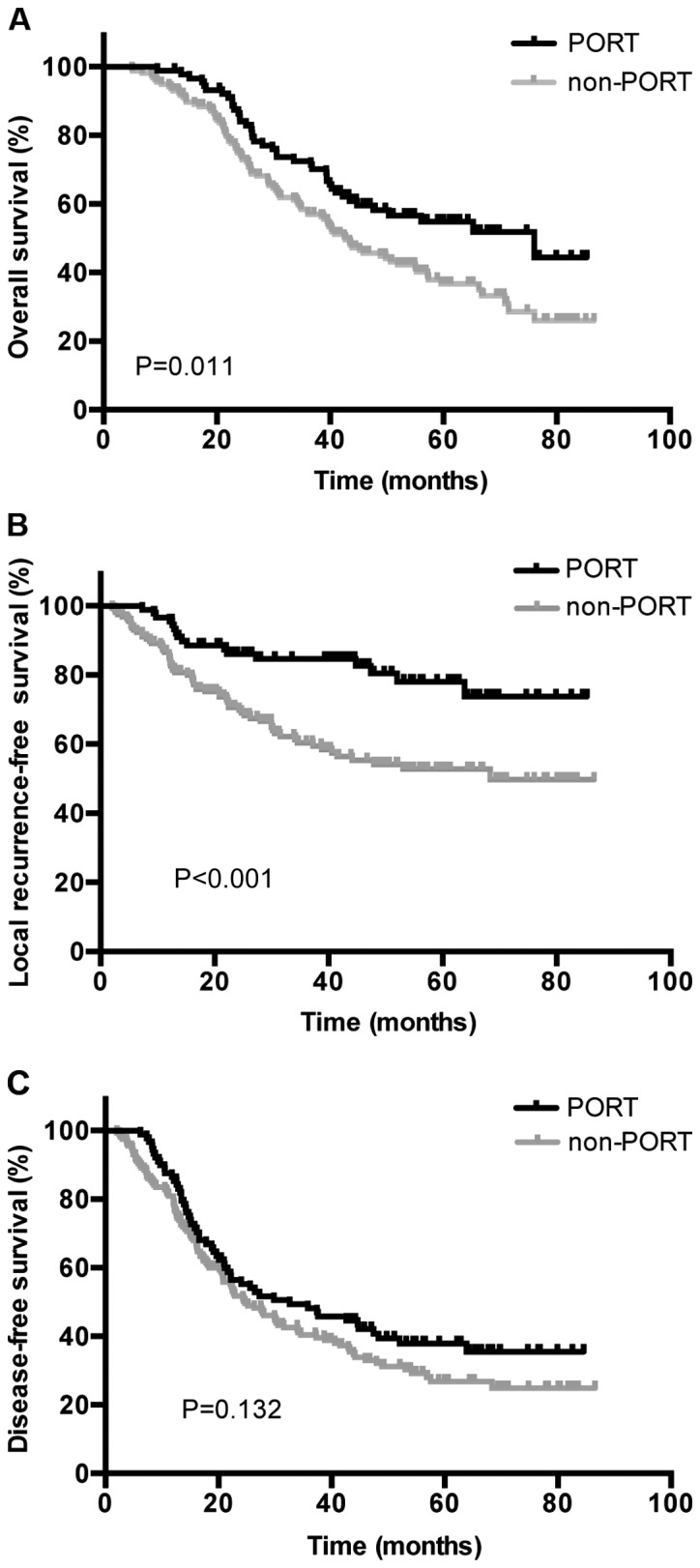
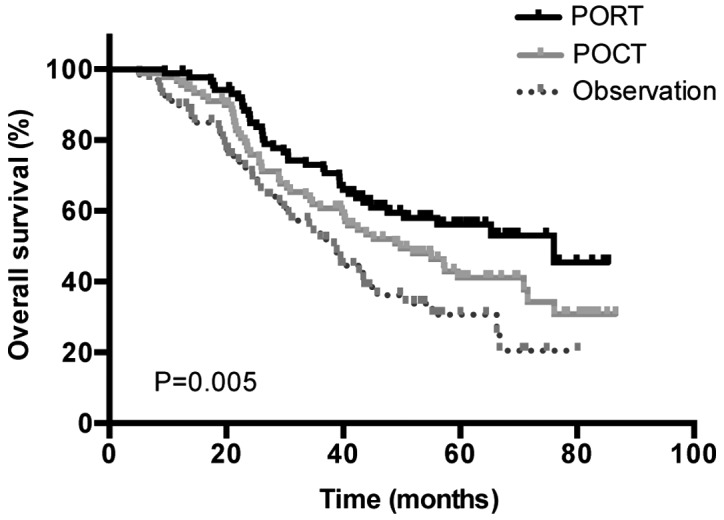
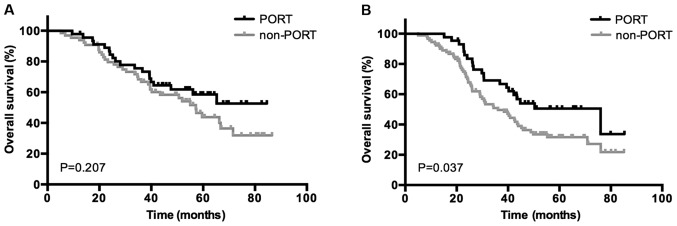
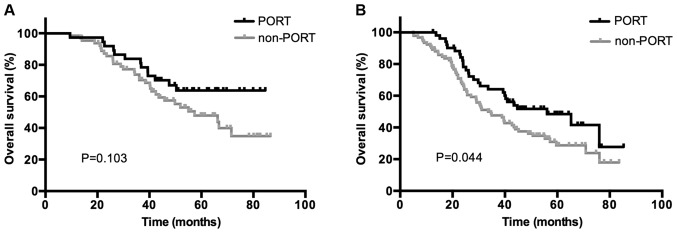
The function of postoperative radiotherapy (PORT) in patients with completely resected pathologically N2 (pN2) non-small cell lung cancer (NSCLC) remains controversial due to a lack of prospective studies. The present study aimed to evaluate the efficacy of PORT in completely resected pN2 NSCLC when using modern radiation techniques, and to determine the associations between clinicopathological factors and PORT and survival rates. Following patient selection, 246 out of 269 consecutive patients with pN2 NSCLC were enrolled in the present study, with 88 patients having received postoperative chemotherapy (POCT) and PORT, 90 having received adjuvant chemotherapy, 1 having received adjuvant radiotherapy and the remaining 67 having received no adjuvant therapy. Overall survival (OS), local recurrence-free survival (LRFS) and disease-free survival (DFS) were estimated using the Kaplan-Meier method. The median age of the patients was 59 years, overall, 175 (71.1%) of the patients were male and the median radiation dose was 50.4 Gy. The median follow-up duration was 38.3 months. The 1-, 3- and 5-year OS rates were 98.9, 71.3 and 54.9%, and 93.0, 58.4 and 36.7% (P=0.011) in the PORT and non-PORT group, respectively. The 1-, 3- and 5-year LRFS rates were 95.5, 84.6 and 78.0%, and 86.6, 70.6 and 52.8% (P<0.001) in the PORT and non-PORT groups, respectively. The 1-, 3- and 5-year DFS rates were 86.5, 55.2 and 37.9%, and 80.9, 40.3 and 26.8% (P=0.132) in the PORT and non-PORT groups, respectively. Univariate analysis revealed that the OS rate was significantly increased in patients with peripheral tumors (P=0.029), pT1-2 (P=0.015), one N2 lymph node (LN) metastasis (P=0.001), single N2 station metastasis (P=0.030), no bronchial involvement (P=0.025), use of PORT (P=0.011) and POCT (P=0.003). Multivariate analysis revealed that PORT (HR, 0.755; 95% CI, 0.498-0.986; P=0.047), POCT (HR, 0.645; 95% CI, 0.420-0.988; P=0.044), bronchial involvement (HR, 1.453; 95% CI, 1.002-2.107; P=0.049) and ≥2 N2 metastases (HR, 1.969; 95% CI, 1.228-3.157; P=0.005) were significant independent predictors of OS. Subgroup analysis demonstrated an increased OS rate with PORT only in the patients with positive bronchial involvement and ≥2 N2 LN metastases. The results revealed that PORT may improve the LRFS and OS rates in completely resected pN2 NSCLC, and that the patients with positive bronchial involvement and ≥2 N2 LN metastases may receive more benefit from PORT.
Keywords: clinicopathological factors; non-small cell lung cancer; overall survival; postoperative radiotherapy; prognostic factors.
Figures
References
-
- Goeckenjan G, Sitter H, Thomas M, Branscheid D, Flentje M, Griesinger F, Niederle N, Stuschke M, Blum T, Deppermann KM, et al. Prevention, diagnosis, therapy, and follow-up of lung cancer: Interdisciplinary guideline of the German Respiratory Society and the German Cancer Society. Pneumologie. 2011;65:39–59. doi: 10.1055/s-0030-1255961. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources