

Effect of a machine learning-based severe sepsis prediction algorithm on patient survival and hospital length of stay: a randomised clinical trial
- PMID: 29435343
- PMCID: PMC5687546
- DOI: 10.1136/bmjresp-2017-000234
Effect of a machine learning-based severe sepsis prediction algorithm on patient survival and hospital length of stay: a randomised clinical trial
Abstract
Introduction: Several methods have been developed to electronically monitor patients for severe sepsis, but few provide predictive capabilities to enable early intervention; furthermore, no severe sepsis prediction systems have been previously validated in a randomised study. We tested the use of a machine learning-based severe sepsis prediction system for reductions in average length of stay and in-hospital mortality rate.
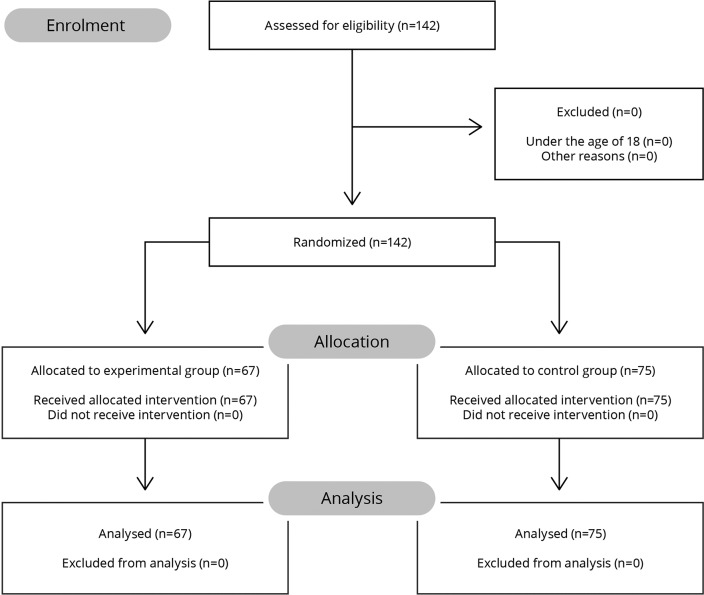
Methods: We conducted a randomised controlled clinical trial at two medical-surgical intensive care units at the University of California, San Francisco Medical Center, evaluating the primary outcome of average length of stay, and secondary outcome of in-hospital mortality rate from December 2016 to February 2017. Adult patients (18+) admitted to participating units were eligible for this factorial, open-label study. Enrolled patients were assigned to a trial arm by a random allocation sequence. In the control group, only the current severe sepsis detector was used; in the experimental group, the machine learning algorithm (MLA) was also used. On receiving an alert, the care team evaluated the patient and initiated the severe sepsis bundle, if appropriate. Although participants were randomly assigned to a trial arm, group assignments were automatically revealed for any patients who received MLA alerts.
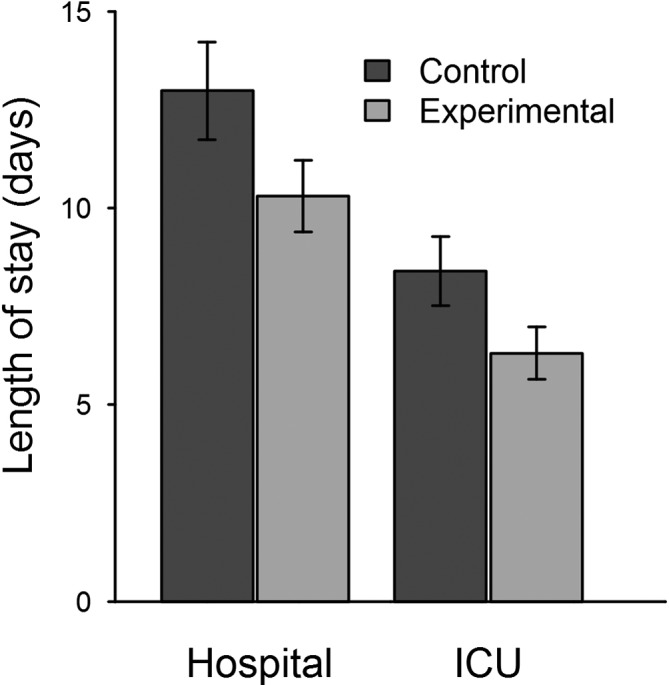
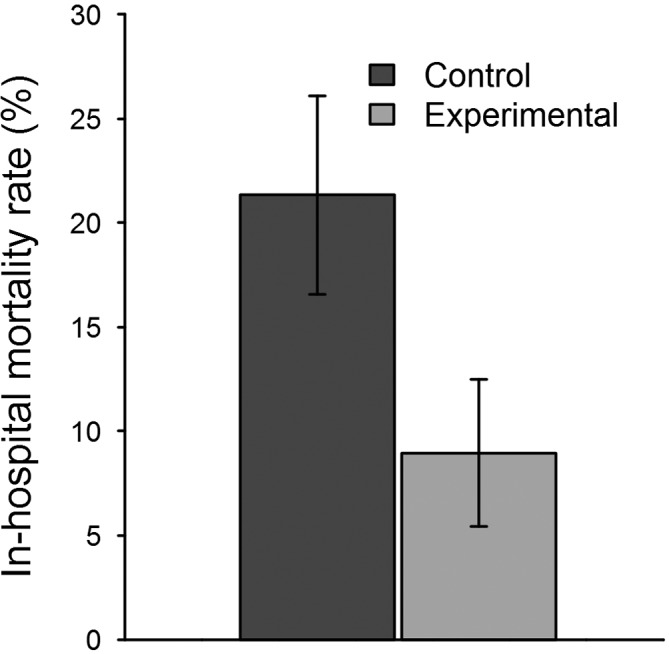
Results: Outcomes from 75 patients in the control and 67 patients in the experimental group were analysed. Average length of stay decreased from 13.0 days in the control to 10.3 days in the experimental group (p=0.042). In-hospital mortality decreased by 12.4 percentage points when using the MLA (p=0.018), a relative reduction of 58.0%. No adverse events were reported during this trial.
Conclusion: The MLA was associated with improved patient outcomes. This is the first randomised controlled trial of a sepsis surveillance system to demonstrate statistically significant differences in length of stay and in-hospital mortality.
Trial registration: NCT03015454.
Keywords: alerts; electronic health records; machine learning; patient monitoring; prediction; sepsis; severe sepsis.
Conflict of interest statement
Competing interests: SM and RD are employees of Dascena. CB reports receiving consulting fees from Dascena. CB, DS and MF report receiving research grant funding from Dascena.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303–10. doi:10.1097/00003246-200107000-00002 - DOI - PubMed
-
- Chalupka AN, Talmor D. The economics of sepsis. Crit Care Clin 2012;28:57–76. doi:10.1016/j.ccc.2011.09.003 - DOI - PubMed
-
- Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for Sepsis and Septic Shock (sepsis-3). JAMA 2016;315:801–10. doi:10.1001/jama.2016.0287 - DOI - PMC - PubMed
-
- Henry KE, Hager DN, Pronovost PJ, et al. A Targeted Real-time Early Warning Score (TREWScore) for septic shock. Sci Transl Med 2015;7:299ra122 doi:10.1126/scitranslmed.aab3719 - DOI - PubMed
-
- Lever A, Mackenzie I. Sepsis: definition, epidemiology, and diagnosis. BMJ 2007;335:879–83. doi:10.1136/bmj.39346.495880.AE - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical