

Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients
- PMID: 29436178
- PMCID: PMC5852359
- DOI: 10.1002/cam4.1372
Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients
Erratum in
-
Corrigendum.Cancer Med. 2018 Jun;7(6):2792. doi: 10.1002/cam4.1593. Cancer Med. 2018. PMID: 29924501 Free PMC article. No abstract available.
Abstract
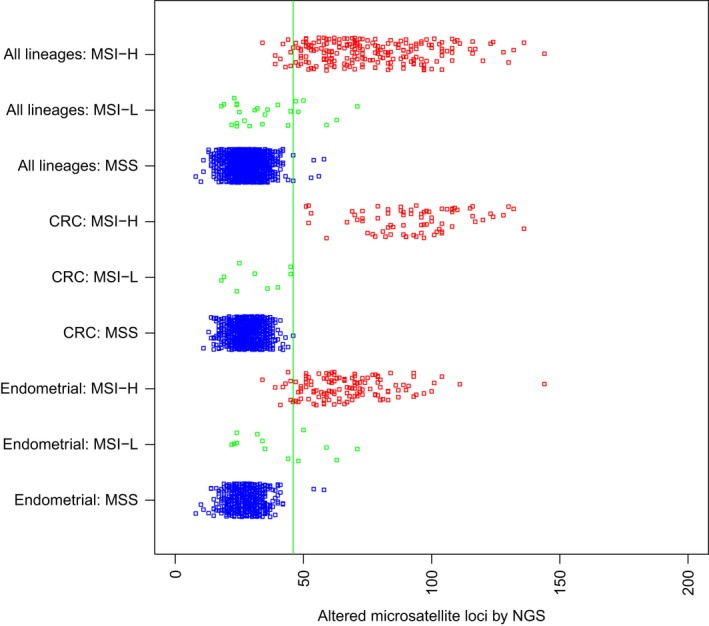
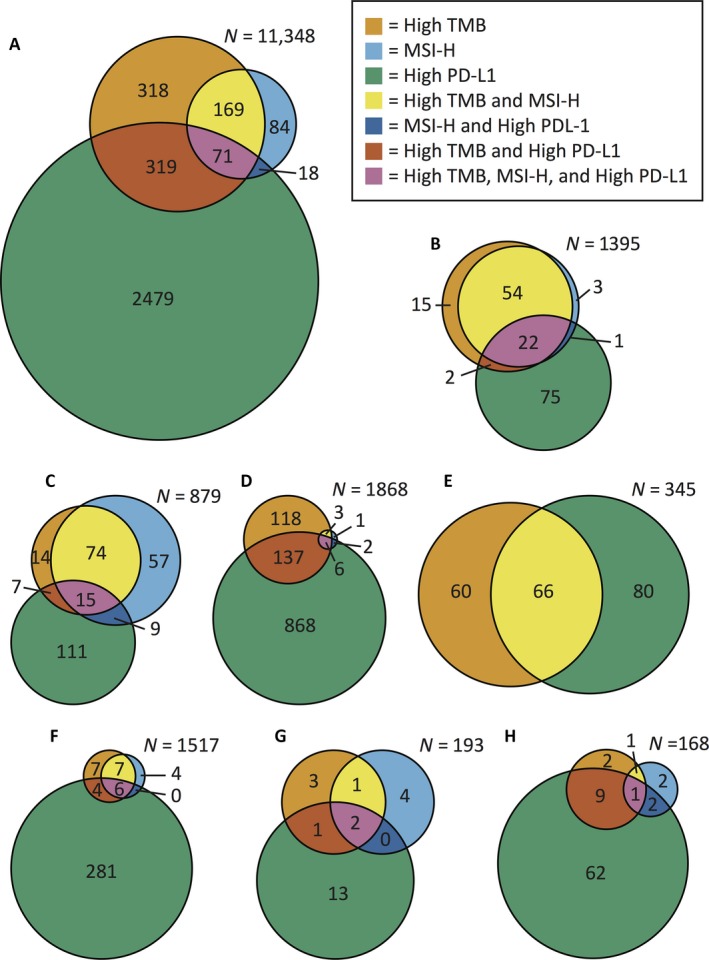
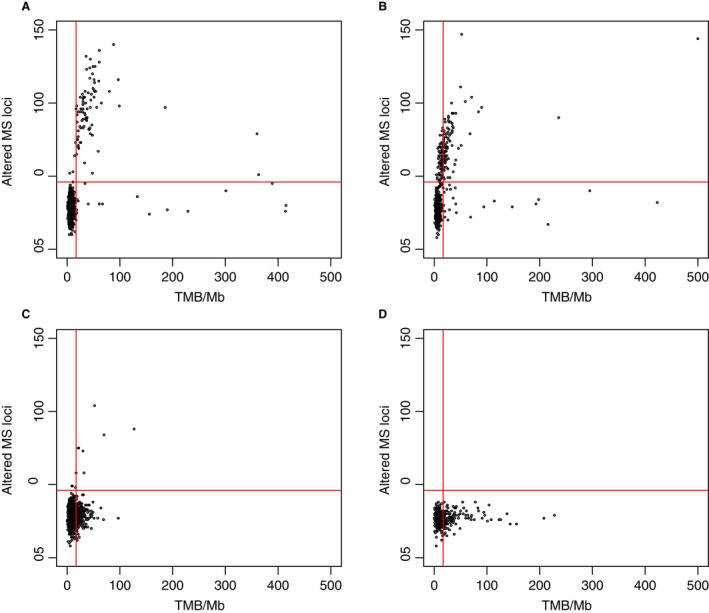
Microsatellite instability (MSI) testing identifies patients who may benefit from immune checkpoint inhibitors. We developed an MSI assay that uses data from a commercially available next-generation sequencing (NGS) panel to determine MSI status. The assay is applicable across cancer types and does not require matched samples from normal tissue. Here, we describe the MSI-NGS method and explore the relationship of MSI with tumor mutational burden (TMB) and PD-L1. MSI examined by PCR fragment analysis and NGS was compared for 2189 matched cases. Mismatch repair status by immunohistochemistry was compared to MSI-NGS for 1986 matched cases. TMB was examined by NGS, and PD-L1 was determined by immunohistochemistry. Among 2189 matched cases that spanned 26 cancer types, MSI-NGS, as compared to MSI by PCR fragment analysis, had sensitivity of 95.8% (95% confidence interval [CI] 92.24, 98.08), specificity of 99.4% (95% CI 98.94, 99.69), positive predictive value of 94.5% (95% CI 90.62, 97.14), and negative predictive value of 99.2% (95% CI, 98.75, 99.57). High MSI (MSI-H) status was identified in 23 of 26 cancer types. Among 11,348 cases examined (including the 2189 matched cases), the overall rates of MSI-H, TMB-high, and PD-L1 positivity were 3.0%, 7.7%, and 25.4%, respectively. Thirty percent of MSI-H cases were TMB-low, and only 26% of MSI-H cases were PD-L1 positive. The overlap between TMB, MSI, and PD-L1 differed among cancer types. Only 0.6% of the cases were positive for all three markers. MSI-H status can be determined by NGS across cancer types. MSI-H offers distinct data for treatment decisions regarding immune checkpoint inhibitors, in addition to the data available from TMB and PD-L1.
Keywords: Antineoplastic agents/therapeutic use; DNA mismatch repair; checkpoint inhibitor; microsatellite instability; next-generation sequencing; precision medicine; programmed cell death 1 receptor/antagonists and inhibitors.
© 2018 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
References
-
- Hause, R. J. , Pritchard C. C., Shendure J., and Salipante S. J.. 2016. Classification and characterization of microsatellite instability across 18 cancer types. Nat. Med. 22:1342–1350. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
