

Transplant-Free Survival and Interventions at 6 Years in the SVR Trial
- PMID: 29437119
- PMCID: PMC5963989
- DOI: 10.1161/CIRCULATIONAHA.117.029375
Transplant-Free Survival and Interventions at 6 Years in the SVR Trial
Abstract
Background: In the SVR trial (Single Ventricle Reconstruction), 1-year transplant-free survival was better for the Norwood procedure with right ventricle-to-pulmonary artery shunt (RVPAS) compared with a modified Blalock-Taussig shunt in patients with hypoplastic left heart and related syndromes. At 6 years, we compared transplant-free survival and other outcomes between the groups.
Methods: Medical history was collected annually using medical record review, telephone interviews, and the death index. The cohort included 549 patients randomized and treated in the SVR trial.
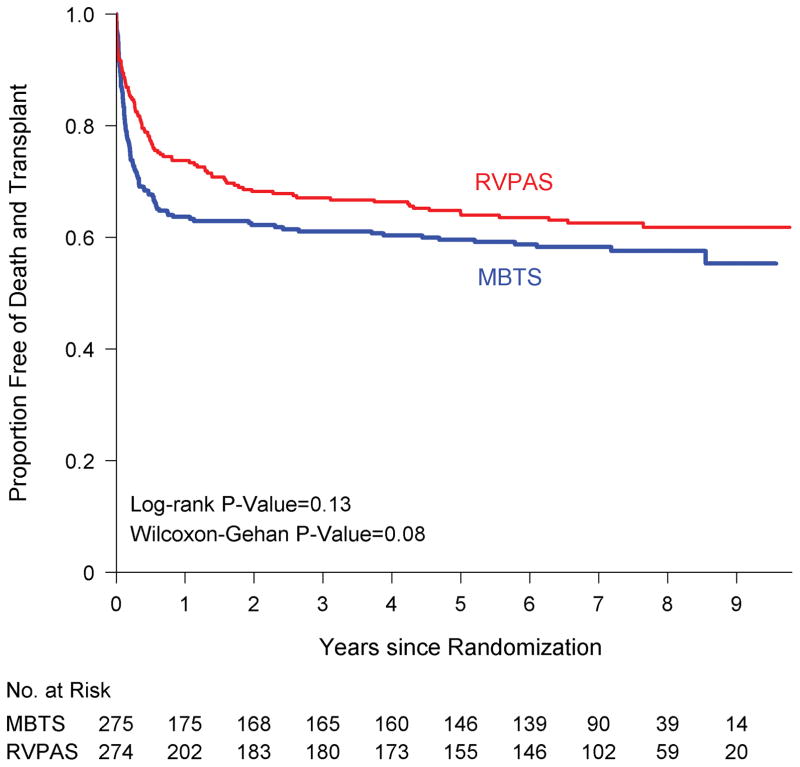
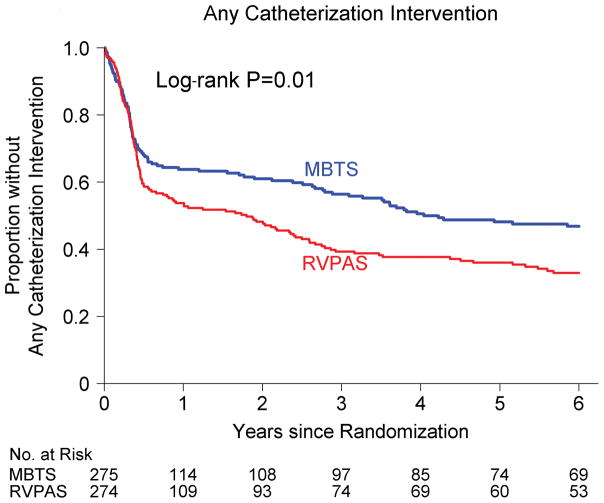
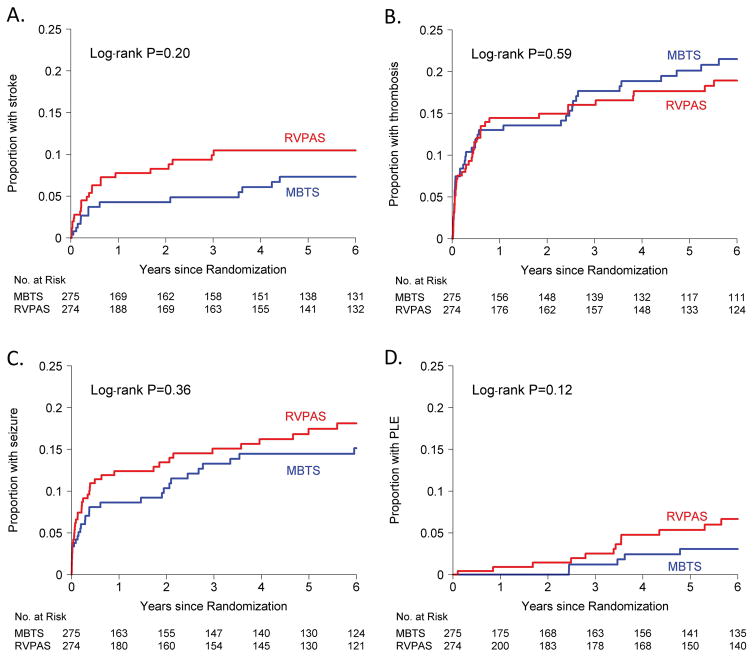
Results: Transplant-free survival for the RVPAS versus modified Blalock-Taussig shunt groups did not differ at 6 years (64% versus 59%, P=0.25) or with all available follow-up of 7.1±1.6 years (log-rank P=0.13). The RVPAS versus modified Blalock-Taussig shunt treatment effect had nonproportional hazards (P=0.009); the hazard ratio (HR) for death or transplant favored the RVPAS before stage II surgery (HR, 0.66; 95% confidence interval, 0.48-0.92). The effect of shunt type on death or transplant was not statistically significant between stage II to Fontan surgery (HR, 1.36; 95% confidence interval, 0.86-2.17; P=0.17) or after the Fontan procedure (HR, 0.76; 95% confidence interval, 0.33-1.74; P=0.52). By 6 years, patients with RVPAS had a higher incidence of catheter interventions (0.38 versus 0.23/patient-year, P<0.001), primarily because of more interventions between the stage II and Fontan procedures (HR, 1.72; 95% confidence interval, 1.00-3.03). Complications did not differ by shunt type; by 6 years, 1 in 5 patients had had a thrombotic event, and 1 in 6 had had seizures.
Conclusions: By 6 years, the hazards of death or transplant and catheter interventions were not different between the RVPAS versus modified Blalock-Taussig shunt groups. Children assigned to the RVPAS group had 5% higher transplant-free survival, but the difference did not reach statistical significance, and they required more catheter interventions. Both treatment groups have accrued important complications.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00115934.
Keywords: Norwood procedure; cardiac surgery; congenital heart defect; congenital heart disease; single ventricle.
© 2018 American Heart Association, Inc.
Conflict of interest statement
No relevant conflicts to disclose.
Figures
Comment in
-
Surgical Palliation for Hypoplastic Left Heart Syndrome: For Now, Just Keep Doing What You Do Best.Circulation. 2018 May 22;137(21):2254-2255. doi: 10.1161/CIRCULATIONAHA.118.033689. Circulation. 2018. PMID: 29784679 No abstract available.
-
On rough road of hypoplastic left heart syndrome after Norwood procedure.J Thorac Dis. 2019 Mar;11(Suppl 3):S465-S467. doi: 10.21037/jtd.2018.11.27. J Thorac Dis. 2019. PMID: 30997249 Free PMC article. No abstract available.
-
Single-ventricle reconstruction 2.0: A closer look at our understanding of care for infants undergoing the Norwood procedure.J Thorac Cardiovasc Surg. 2019 Sep;158(3):837-842.e5. doi: 10.1016/j.jtcvs.2018.12.121. Epub 2019 Apr 17. J Thorac Cardiovasc Surg. 2019. PMID: 31101343 No abstract available.
References
-
- Norwood WI, Kirklin JK, Sanders SP. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. 1980;45:87–91. - PubMed
-
- Sano S, Ishino K, Kawada M, Arai S, Kasahara S, Asai T, Masuda Z, Takeuchi M, Ohtsuki S. Right ventricle-pulmonary artery shunt in first-stage palliation of hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 2003;126:504–509. - PubMed
-
- Ohye RG, Sleeper LA, Mahony L, Newburger JW, Pearson GD, Lu M, Goldberg CS, Tabbutt S, Frommelt PC, Ghanayem NS, Laussen PC, Rhodes JF, Lewis AB, Mital S, Ravishankar C, Williams IA, Dunbar-Masterson C, Atz AM, Colan S, Minich LL, Pizarro C, Kanter KR, Jaggers J, Jacobs JP, Krawczeski CD, Pike N, McCrindle BW, Virzi L, Gaynor JW. Comparison of shunt types in the Norwood procedure for single-ventricle lesions. N Engl J Med. 2010;362:1980–1992. - PMC - PubMed
-
- Newburger JW, Sleeper LA, Frommelt PC, Pearson GD, Mahle WT, Chen S, Dunbar-Masterson C, Mital S, Williams IA, Ghanayem NS, Goldberg CS, Jacobs JP, Krawczeski CD, Lewis AB, Pasquali SK, Pizarro C, Gruber PJ, Atz AM, Khaikin S, Gaynor JW, Ohye RG Pediatric Heart Network I. Transplantation-free survival and interventions at 3 years in the single ventricle reconstruction trial. Circulation. 2014;129:2013–2020. - PMC - PubMed
-
-
www.pediatricheartnetwork.org/ForResearchers/PHNPublicUseDatasets.PHN Public Use Datasets website.
-
Publication types
MeSH terms
Associated data
Grants and funding
- UG1 HL135646/HL/NHLBI NIH HHS/United States
- UG1 HL135685/HL/NHLBI NIH HHS/United States
- U01 HL068269/HL/NHLBI NIH HHS/United States
- U01 HL068279/HL/NHLBI NIH HHS/United States
- UG1 HL135689/HL/NHLBI NIH HHS/United States
- U01 HL068290/HL/NHLBI NIH HHS/United States
- UG1 HL135682/HL/NHLBI NIH HHS/United States
- U01 HL068288/HL/NHLBI NIH HHS/United States
- U10 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068281/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068292/HL/NHLBI NIH HHS/United States
- U01 HL085057/HL/NHLBI NIH HHS/United States
- U10 HL109778/HL/NHLBI NIH HHS/United States
- UG1 HL135678/HL/NHLBI NIH HHS/United States
- U01 HL068285/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
