

Agalsidase alfa versus agalsidase beta for the treatment of Fabry disease: an international cohort study
- PMID: 29437868
- PMCID: PMC5931248
- DOI: 10.1136/jmedgenet-2017-104863
Agalsidase alfa versus agalsidase beta for the treatment of Fabry disease: an international cohort study
Abstract
Background: Two recombinant enzymes (agalsidase alfa 0.2 mg/kg/every other week and agalsidase beta 1.0 mg/kg/every other week) have been registered for the treatment of Fabry disease (FD), at equal high costs. An independent international initiative compared clinical and biochemical outcomes of the two enzymes.
Methods: In this multicentre retrospective cohort study, clinical event rate, left ventricular mass index (LVMI), estimated glomerular filtration rate (eGFR), antibody formation and globotriaosylsphingosine (lysoGb3) levels were compared between patients with FD treated with agalsidase alfa and beta at their registered dose after correction for phenotype and sex.
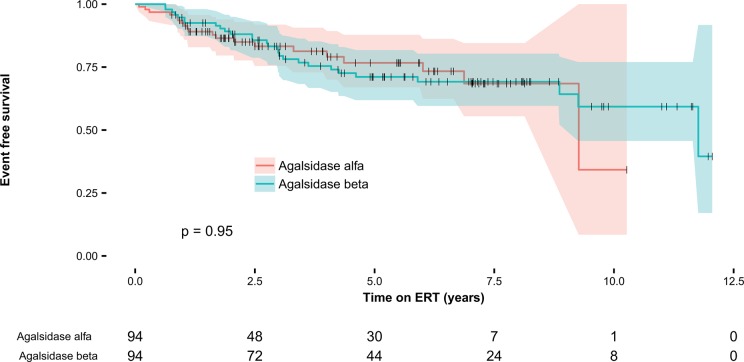
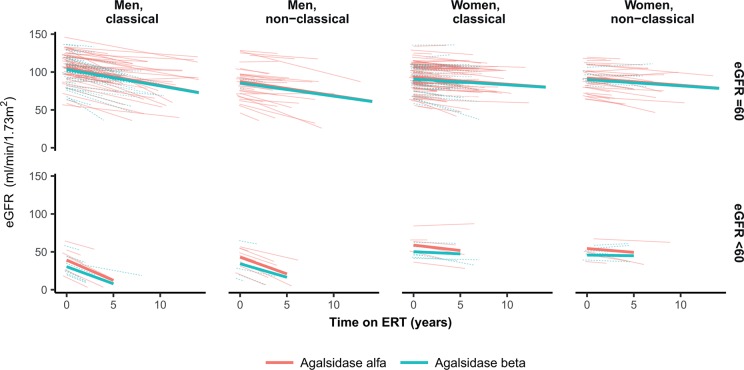
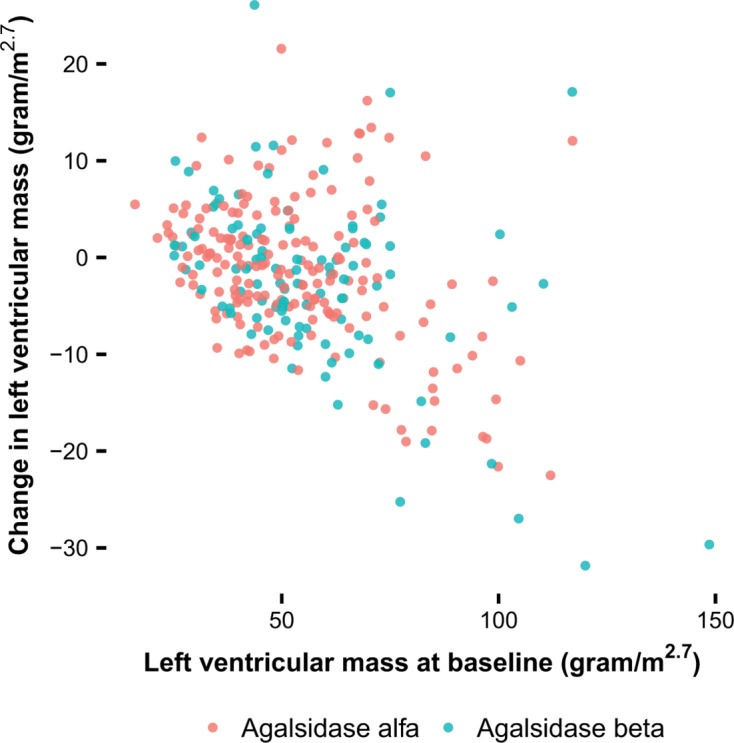
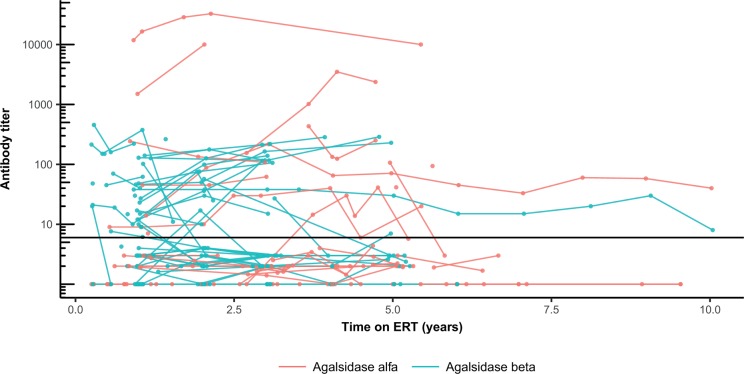
Results: 387 patients (192 women) were included, 248 patients received agalsidase alfa. Mean age at start of enzyme replacement therapy was 46 (±15) years. Propensity score matched analysis revealed a similar event rate for both enzymes (HR 0.96, P=0.87). The decrease in plasma lysoGb3 was more robust following treatment with agalsidase beta, specifically in men with classical FD (β: -18 nmol/L, P<0.001), persisting in the presence of antibodies. The risk to develop antibodies was higher for patients treated with agalsidase beta (OR 2.8, P=0.04). LVMI decreased in a higher proportion following the first year of agalsidase beta treatment (OR 2.27, P=0.03), while eGFR slopes were similar.
Conclusions: Treatment with agalsidase beta at higher dose compared with agalsidase alfa does not result in a difference in clinical events, which occurred especially in those with more advanced disease. A greater biochemical response, also in the presence of antibodies, and better reduction in left ventricular mass was observed with agalsidase beta.
Keywords: agalsidase alfa; agalsidase beta; enzyme replacement therapy; ert; fabry disease.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: CW has received honoraria for lecturing from Sanofi Genzyme (Cambridge, Massachusetts, USA) and a grant to the institution from Sanofi Genzyme and Shire (Dublin, Ireland). SS, DGB, AK, MI and MLW have served on advisory boards, received fees for speaking or travel support and participated in other clinical trials and registries sponsored by Sanofi Genzyme and Shire. MLW has received travel funds, research funds or consultancy fees from Actelion, Alexion, Amicus, Excelsior, GlaxoSmithKline, Protalix and SumitomoPharma. AM has received honoraria for consultancies and educational activities as well as research support from Shire, Sanofi Genzyme, Protalix/Pfizer (New York City, New York, USA) and Amicus. DO has received speakers honoraria from Sanofi Genzyme and travel assistance from Sanofi Genzyme and Shire. PME has received speaker fees from Shire and consultancy and speaker fees from Sanofi Genzyme, Pfizer and Gilead Sciences (Foster City, California, USA). DAH has received honoraria for speaking and participating in advisory boards and support for research from Shire, Sanofi Genzyme, Amicus (Cranbury, New Jersey, USA) and Protalix (Carmiel, Israel). Also, DAH has a consultancy arrangement through UCL Consultants (London, UK) to support, in part, laboratory research. MB and CEMH have received travel support, honoraria for consultancies and educational grants from Sanofi Genzyme, Shire, Protalix, Actelion (Allschwil, Switzerland) and Amicus. All financial arrangements are made with the AMC Medical Research BV in accordance with the Research Code of the Academic Medical Center.
Figures


References
-
- Desnick RJ, Ioannou YA, Eng CM, et al. . Α-galactosidase a deficiency: fabry disease : Valle D, Beaudet AL, Vogelstein B, Kinzler KW, Antonarakis SE, Ballabio A, Gibson KMG, OMMBID - The Online Metabolic and Molecular Bases of Inherited Diseases. New York: McGraw-Hill, 2013.
-
- Aerts JM, Groener JE, Kuiper S, Donker-Koopman WE, Strijland A, Ottenhoff R, van Roomen C, Mirzaian M, Wijburg FA, Linthorst GE, Vedder AC, Rombach SM, Cox-Brinkman J, Somerharju P, Boot RG, Hollak CE, Brady RO, Poorthuis BJ. Elevated globotriaosylsphingosine is a hallmark of Fabry disease. Proc Natl Acad Sci U S A 2008;105:2812–7. 10.1073/pnas.0712309105 - DOI - PMC - PubMed
-
- Dekker N, van Dussen L, Hollak CE, Overkleeft H, Scheij S, Ghauharali K, van Breemen MJ, Ferraz MJ, Groener JE, Maas M, Wijburg FA, Speijer D, Tylki-Szymanska A, Mistry PK, Boot RG, Aerts JM. Elevated plasma glucosylsphingosine in Gaucher disease: relation to phenotype, storage cell markers, and therapeutic response. Blood 2011;118:e118–27. 10.1182/blood-2011-05-352971 - DOI - PMC - PubMed
-
- van der Tol L, Cassiman D, Houge G, Janssen MC, Lachmann RH, Linthorst GE, Ramaswami U, Sommer C, Tøndel C, West ML, Weidemann F, Wijburg FA, Svarstad E, Hollak CE, Biegstraaten M. Uncertain diagnosis of fabry disease in patients with neuropathic pain, angiokeratoma or cornea verticillata: consensus on the approach to diagnosis and follow-up. JIMD Rep 2014;17:83–90. 10.1007/8904_2014_342 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous