

Integrative analysis of exogenous, endogenous, tumour and immune factors for precision medicine
- PMID: 29437869
- PMCID: PMC5943183
- DOI: 10.1136/gutjnl-2017-315537
Integrative analysis of exogenous, endogenous, tumour and immune factors for precision medicine
Abstract
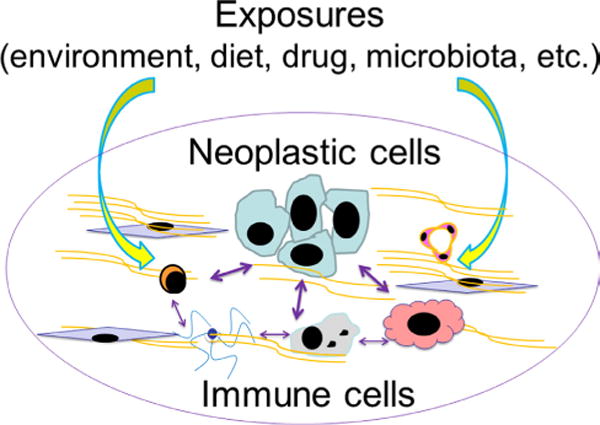
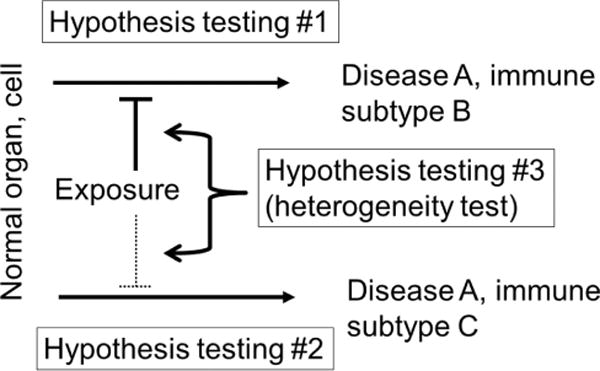
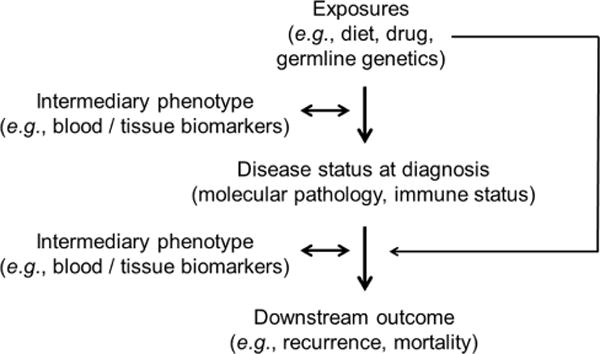
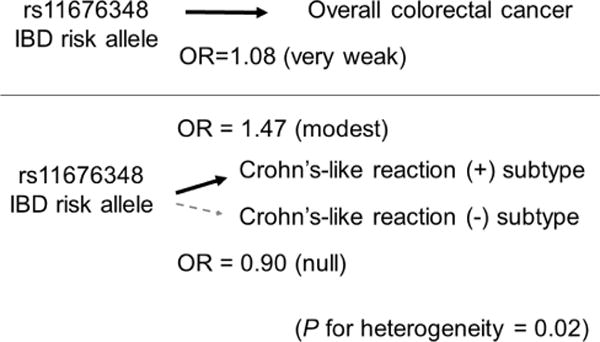
Immunotherapy strategies targeting immune checkpoints such as the CTLA4 and CD274 (programmed cell death 1 ligand 1, PD-L1)/PDCD1 (programmed cell death 1, PD-1) T-cell coreceptor pathways are revolutionising oncology. The approval of pembrolizumab use for solid tumours with high-level microsatellite instability or mismatch repair deficiency by the US Food and Drug Administration highlights promise of precision immuno-oncology. However, despite evidence indicating influences of exogenous and endogenous factors such as diet, nutrients, alcohol, smoking, obesity, lifestyle, environmental exposures and microbiome on tumour-immune interactions, integrative analyses of those factors and immunity lag behind. Immune cell analyses in the tumour microenvironment have not adequately been integrated into large-scale studies. Addressing this gap, the transdisciplinary field of molecular pathological epidemiology (MPE) offers research frameworks to integrate tumour immunology into population health sciences, and link the exposures and germline genetics (eg, HLA genotypes) to tumour and immune characteristics. Multilevel research using bioinformatics, in vivo pathology and omics (genomics, epigenomics, transcriptomics, proteomics and metabolomics) technologies is possible with use of tissue, peripheral blood circulating cells, cell-free plasma, stool, sputum, urine and other body fluids. This immunology-MPE model can synergise with experimental immunology, microbiology and systems biology. GI neoplasms represent exemplary diseases for the immunology-MPE model, given rich microbiota and immune tissues of intestines, and the well-established carcinogenic role of intestinal inflammation. Proof-of-principle studies on colorectal cancer provided insights into immunomodulating effects of aspirin, vitamin D, inflammatory diets and omega-3 polyunsaturated fatty acids. The integrated immunology-MPE model can contribute to better understanding of environment-tumour-immune interactions, and effective immunoprevention and immunotherapy strategies for precision medicine.
Keywords: cancer Immunobiology; cancer epidemiology; cancer prevention; colorectal carcinoma; molecular pathology.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Galon J, Angell HK, Bedognetti D, et al. The continuum of cancer immunosurveillance: prognostic, predictive, and mechanistic signatures. Immunity. 2013;39:11–26. - PubMed
-
- Smyth MJ, Ngiow SF, Ribas A, et al. Combination cancer immunotherapies tailored to the tumour microenvironment. Nat Rev Clin Oncol. 2016;13:143–58. - PubMed
-
- Mohme M, Riethdorf S, Pantel K. Circulating and disseminated tumour cells - mechanisms of immune surveillance and escape. Nat Rev Clin Oncol. 2017;14:155–67. - PubMed
-
- Gubin MM. Cancer Immunology and Immunotherapy: taking a place in mainstream oncology keystone symposia meeting summary. Cancer Immunol Res. 2017;5:434–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous