

Characterizing the Potency and Impact of Carbon Ion Therapy in a Primary Mouse Model of Soft Tissue Sarcoma
- PMID: 29437879
- PMCID: PMC5912881
- DOI: 10.1158/1535-7163.MCT-17-0965
Characterizing the Potency and Impact of Carbon Ion Therapy in a Primary Mouse Model of Soft Tissue Sarcoma
Abstract
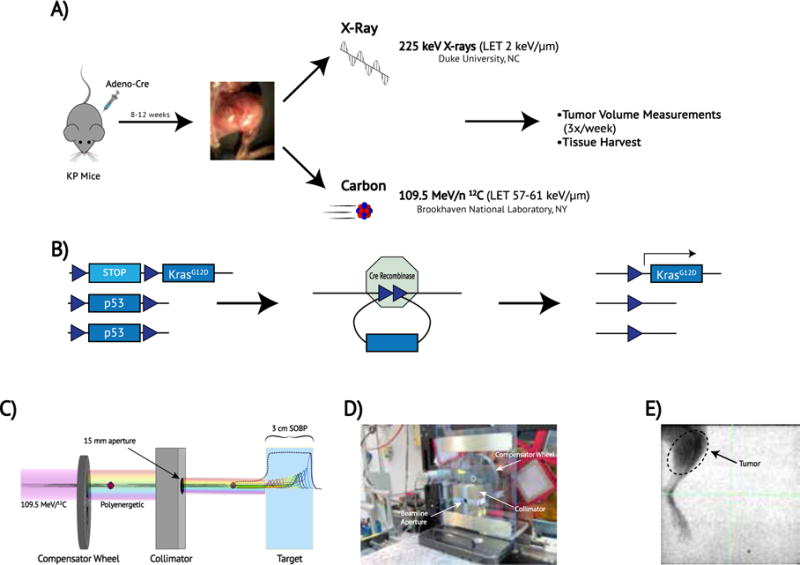
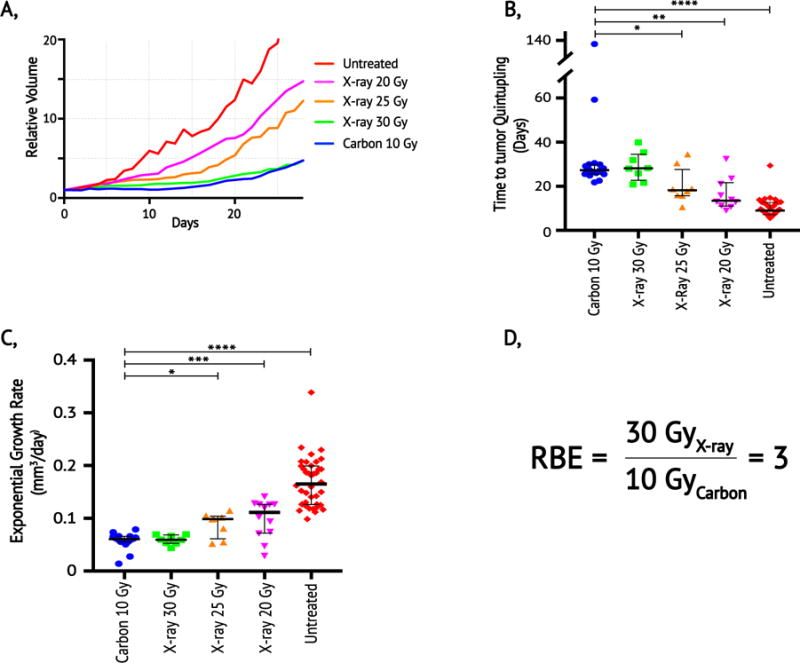
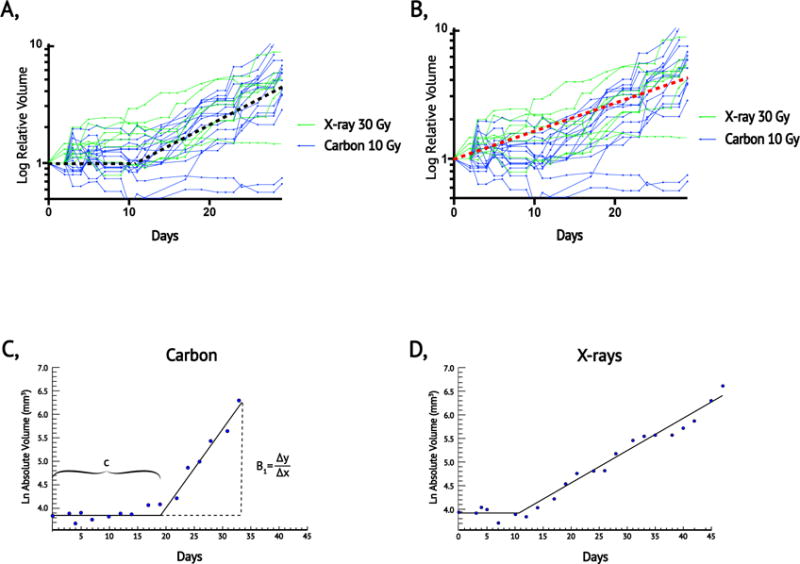
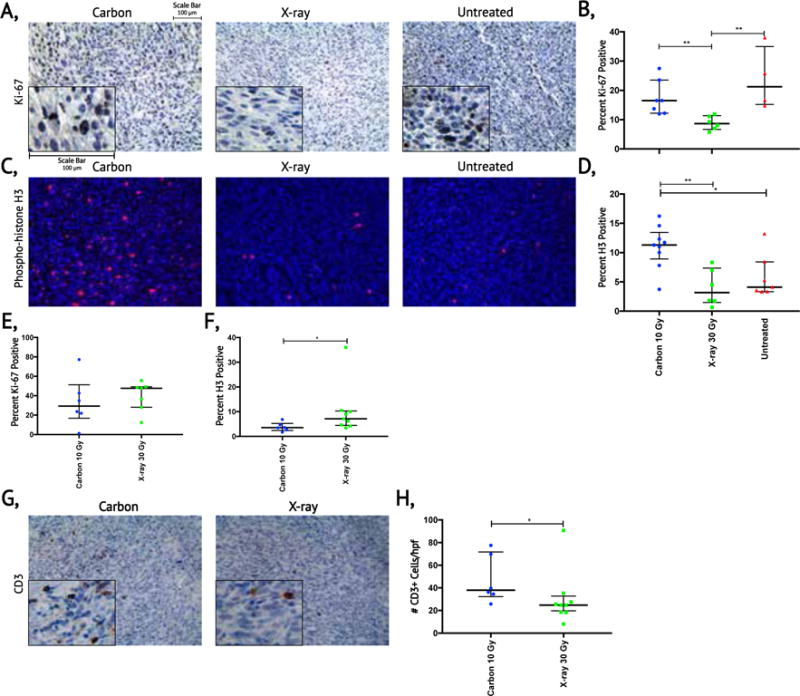
Carbon ion therapy (CIT) offers several potential advantages for treating cancers compared with X-ray and proton radiotherapy, including increased biological efficacy and more conformal dosimetry. However, CIT potency has not been characterized in primary tumor animal models. Here, we calculate the relative biological effectiveness (RBE) of carbon ions compared with X-rays in an autochthonous mouse model of soft tissue sarcoma. We used Cre/loxP technology to generate primary sarcomas in KrasLSL-G12D/+; p53fl/fl mice. Primary tumors were irradiated with a single fraction of carbon ions (10 Gy), X-rays (20 Gy, 25 Gy, or 30 Gy), or observed as controls. The RBE was calculated by determining the dose of X-rays that resulted in similar time to posttreatment tumor volume quintupling and exponential growth rate as 10 Gy carbon ions. The median tumor volume quintupling time and exponential growth rate of sarcomas treated with 10 Gy carbon ions and 30 Gy X-rays were similar: 27.3 and 28.1 days and 0.060 and 0.059 mm3/day, respectively. Tumors treated with lower doses of X-rays had faster regrowth. Thus, the RBE of carbon ions in this primary tumor model is 3. When isoeffective treatments of carbon ions and X-rays were compared, we observed significant differences in tumor growth kinetics, proliferative indices, and immune infiltrates. We found that carbon ions were three times as potent as X-rays in this aggressive tumor model and identified unanticipated differences in radiation response that may have clinical implications. Mol Cancer Ther; 17(4); 858-68. ©2018 AACR.
©2018 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Howlader NNA, Krapcho M, Miller D, Bishop K, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2014. National Cancer Institute; Bethesda, MD: 2016. Novermber 2016 ed.
-
- Page BR, Hudson AD, Brown DW, Shulman AC, Abdel-Wahab M, Fisher BJ, et al. Cobalt, linac, or other: what is the best solution for radiation therapy in developing countries? Int J Radiat Oncol Biol Phys. 2014;89:476–80. - PubMed
-
- Wang X, Krishnan S, Zhang X, Dong L, Briere T, Crane CH, et al. Proton radiotherapy for liver tumors: dosimetric advantages over photon plans. Medical dosimetry: official journal of the American Association of Medical Dosimetrists. 2008;33:259–67. - PubMed
-
- Glimelius B, Isacsson U, Blomquist E, Grusell E, Jung B, Montelius A. Potential gains using high-energy protons for therapy of malignant tumours. Acta Oncol. 1999;38:137–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
