

Modern diagnosis of GERD: the Lyon Consensus
- PMID: 29437910
- PMCID: PMC6031267
- DOI: 10.1136/gutjnl-2017-314722
Modern diagnosis of GERD: the Lyon Consensus
Abstract
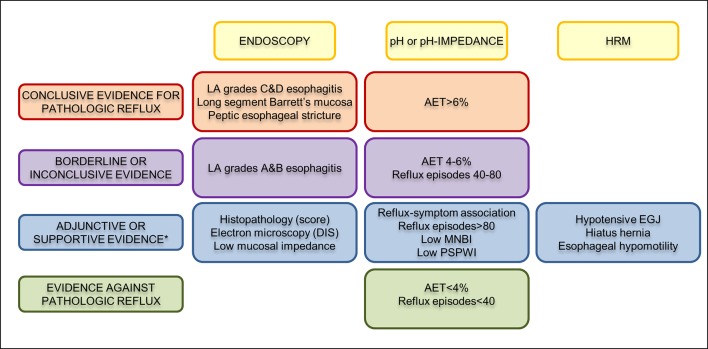
Clinical history, questionnaire data and response to antisecretory therapy are insufficient to make a conclusive diagnosis of GERD in isolation, but are of value in determining need for further investigation. Conclusive evidence for reflux on oesophageal testing include advanced grade erosive oesophagitis (LA grades C and D), long-segment Barrett's mucosa or peptic strictures on endoscopy or distal oesophageal acid exposure time (AET) >6% on ambulatory pH or pH-impedance monitoring. A normal endoscopy does not exclude GERD, but provides supportive evidence refuting GERD in conjunction with distal AET <4% and <40 reflux episodes on pH-impedance monitoring off proton pump inhibitors. Reflux-symptom association on ambulatory reflux monitoring provides supportive evidence for reflux triggered symptoms, and may predict a better treatment outcome when present. When endoscopy and pH or pH-impedance monitoring are inconclusive, adjunctive evidence from biopsy findings (histopathology scores, dilated intercellular spaces), motor evaluation (hypotensive lower oesophageal sphincter, hiatus hernia and oesophageal body hypomotility on high-resolution manometry) and novel impedance metrics (baseline impedance, postreflux swallow-induced peristaltic wave index) can add confidence for a GERD diagnosis; however, diagnosis cannot be based on these findings alone. An assessment of anatomy, motor function, reflux burden and symptomatic phenotype will therefore help direct management. Future GERD management strategies should focus on defining individual patient phenotypes based on the level of refluxate exposure, mechanism of reflux, efficacy of clearance, underlying anatomy of the oesophagogastric junction and psychometrics defining symptomatic presentations.
Keywords: PH monitoring; endoscopy; gastroesophageal reflux disease; manometry.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: CPG: consulting: Ironwood, Torax, Quintiles; teaching and speaking: Medtronic, Diversatek, Reckitt-Benckiser. ES: consulting: AbbVie, Allergan, MSD, Takeda, Sofar, Janssen; teaching and speaking: Medtronic, Reckitt-Benckiser, Malesci, Zambon. FZ: research support: Medtronic, Sandhill Scientific; consulting: Allergan, Reckitt-Benckiser; speaking and teaching: Ipsen Pharma, Biocodex, Coloplast, Takeda, Vifor Pharma, Mayoly Spindler. PJK: consulting: Ironwood. FM: teaching and speaking: Laborie, Medtronic; consulting: Allergan, Endostim. AJPMS: none. MV: Vanderbilt University and Diversatek co-own patent on mucosal impedance technology. DS: research support: Diversatek, Reckitt-Benckiser; OMOM, Jinshan Science & Technology (Group) Co. Ltd., Chongqing, China. MRF: research support: Given Imaging/Covidien, Reckitt Benckiser, Mui Scientific. Educational events: Given Imaging/Covidien, MMS, Sandhill Scientific Instruments. Speaking and teaching: Given Imaging/Covidien, Reckitt Benckiser, Shire, Almirall. MV: consulting: Torax. RT: teaching: Laborie. JT: consulting: Ironwood. AJB: research support: Danone, Bayer; speaking and/or consulting: MMS, Astellas, AstraZeneca, Bayer, Almirall and Allergan. JP: research support: Impleo; speaking and/or consulting: Medtronic, Diversatek, Torax, Ironwood, Takeda, AstraZeneca; stock options: Crospon. SR: research support: Sandhill Scientific, Crospon; teaching: Medtronic; speaker: Mayoly Spindler.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical