

Hydroxychloroquine: A Physiologically-Based Pharmacokinetic Model in the Context of Cancer-Related Autophagy Modulation
- PMID: 29438998
- PMCID: PMC5931434
- DOI: 10.1124/jpet.117.245639
Hydroxychloroquine: A Physiologically-Based Pharmacokinetic Model in the Context of Cancer-Related Autophagy Modulation
Abstract
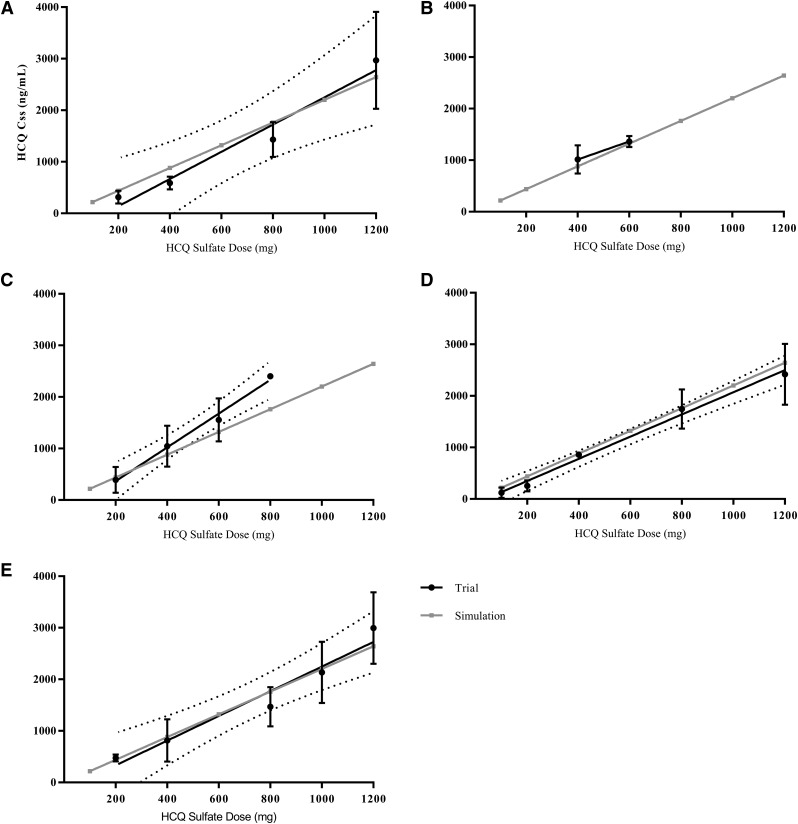
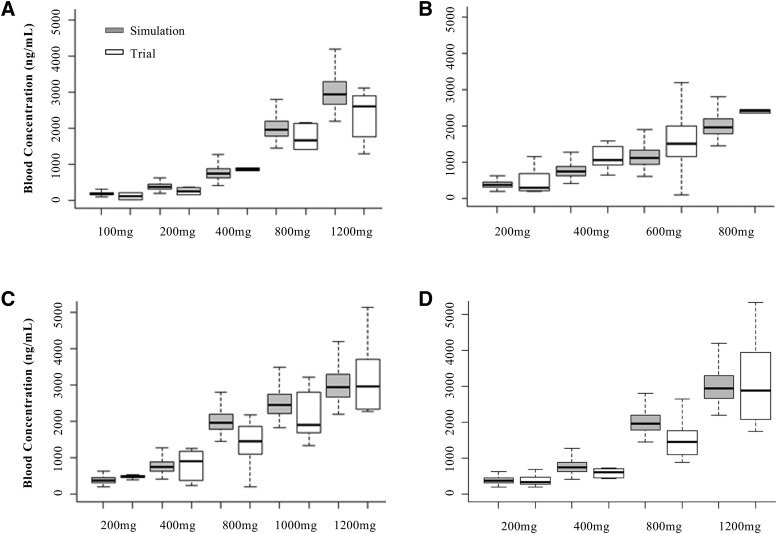
Hydroxychloroquine (HCQ) is a lysosomotropic autophagy inhibitor being used in over 50 clinical trials either alone or in combination with chemotherapy. Pharmacokinetic (PK) and pharmacodynamic (PD) studies with HCQ have shown that drug exposure in the blood does not correlate with autophagy inhibition in either peripheral blood mononuclear cells or tumor tissue. To better explain this PK/PD disconnect, a PBPK was developed for HCQ describing the tissue-specific absorption, distribution, metabolism, and excretion as well as lysosome-specific sequestration. Using physiologic and biochemical parameters derived from literature or obtained experimentally, the model was first developed and validated in mice, and then adapted to simulate human HCQ exposure in whole blood and urine through allometric scaling and species-specific parameter modification. The human model accurately simulated average steady-state concentrations (Css) of those observed in five different HCQ combination clinical trials across seven different doses, which was then expanded by comparison of the Css distribution in a virtual human population at this range of doses. Value of this model lies in its ability to simulate HCQ PK in patients while accounting for PK modification by combination treatment modalities, drug concentrations at the active site in the lysosome under varying pH conditions, and exposure in tissues where toxicity is observed.
Copyright © 2018 by The American Society for Pharmacology and Experimental Therapeutics.
Figures





References
-
- Bischoff KB, Dedrick RL, Zaharko DS, Longstreth JA. (1971) Methotrexate pharmacokinetics. J Pharm Sci 60:1128–1133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
