

Transcriptional Profiling of Synovial Macrophages Using Minimally Invasive Ultrasound-Guided Synovial Biopsies in Rheumatoid Arthritis
- PMID: 29439295
- PMCID: PMC5984677
- DOI: 10.1002/art.40453
Transcriptional Profiling of Synovial Macrophages Using Minimally Invasive Ultrasound-Guided Synovial Biopsies in Rheumatoid Arthritis
Abstract
Objective: Currently, there are no reliable biomarkers for predicting therapeutic response in patients with rheumatoid arthritis (RA). The synovium may unlock critical information for determining efficacy, since a reduction in the numbers of sublining synovial macrophages remains the most reproducible biomarker. Thus, a clinically actionable method for the collection of synovial tissue, which can be analyzed using high-throughput strategies, must become a reality. This study was undertaken to assess the feasibility of utilizing synovial biopsies as a precision medicine-based approach for patients with RA.
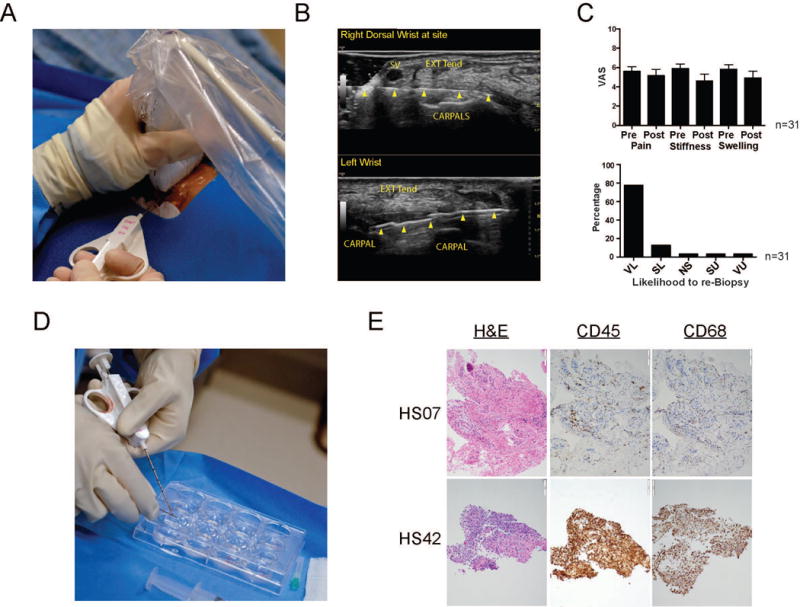
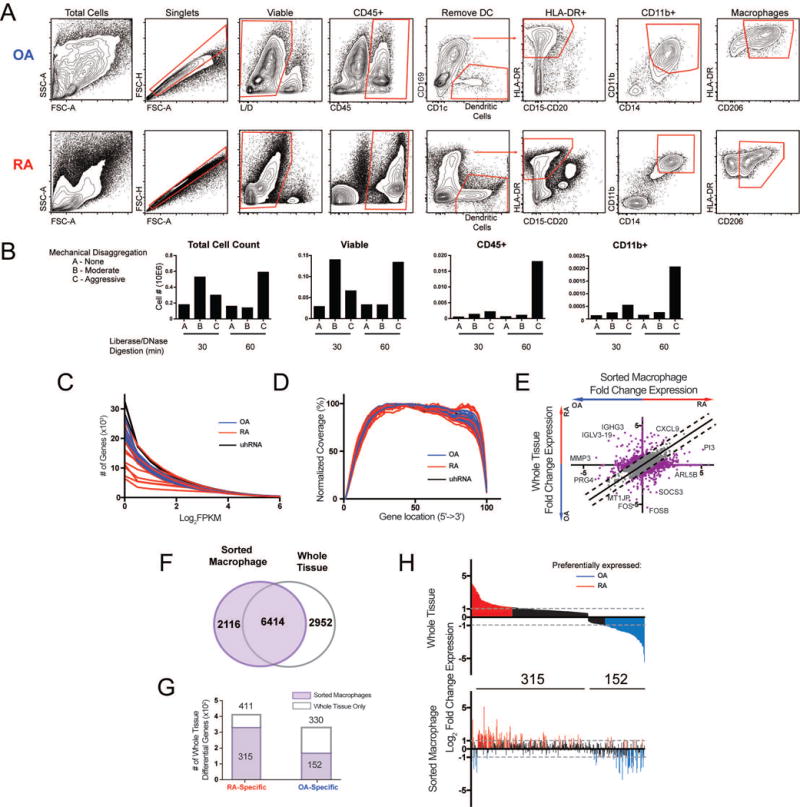
Methods: Rheumatologists at 6 US academic sites were trained in minimally invasive ultrasound-guided synovial tissue biopsy. Biopsy specimens obtained from patients with RA and synovial tissue from patients with osteoarthritis (OA) were subjected to histologic analysis, fluorescence-activated cell sorting, and RNA sequencing (RNA-seq). An optimized protocol for digesting synovial tissue was developed to generate high-quality RNA-seq libraries from isolated macrophage populations. Associations were determined between macrophage transcriptional profiles and clinical parameters in RA patients.
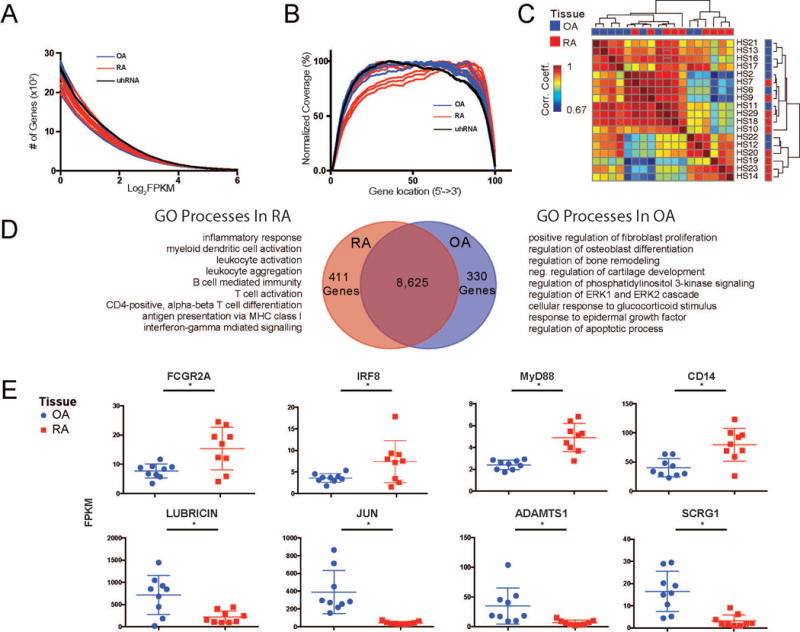
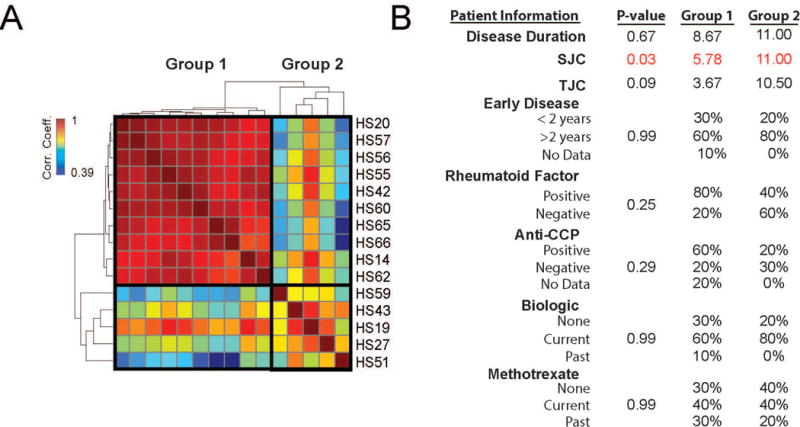
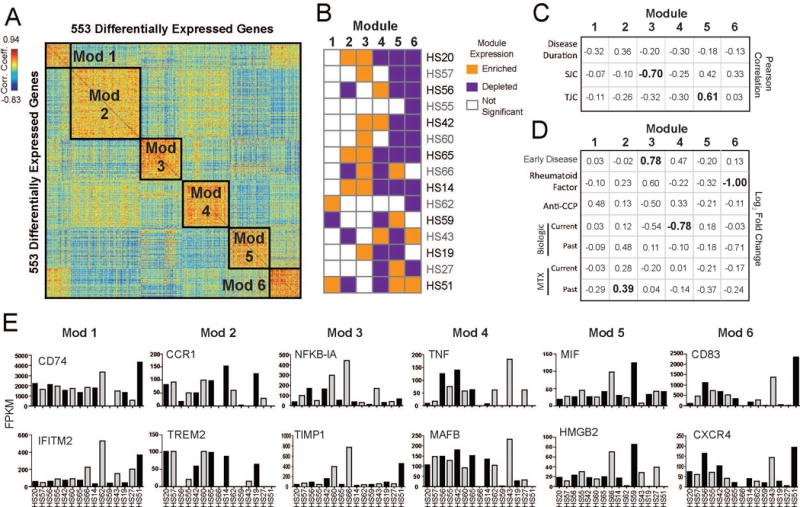
Results: Patients with RA reported minimal adverse effects in response to synovial biopsy. Comparable RNA quality was observed from synovial tissue and isolated macrophages between patients with RA and patients with OA. Whole tissue samples from patients with RA demonstrated a high degree of transcriptional heterogeneity. In contrast, the transcriptional profile of isolated RA synovial macrophages highlighted different subpopulations of patients and identified 6 novel transcriptional modules that were associated with disease activity and therapy.
Conclusion: Performance of synovial tissue biopsies by rheumatologists in the US is feasible and generates high-quality samples for research. Through the use of cutting-edge technologies to analyze synovial biopsy specimens in conjunction with corresponding clinical information, a precision medicine-based approach for patients with RA is attainable.
© 2018, American College of Rheumatology.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Saevarsdottir S, Wallin H, Seddighzadeh M, Ernestam S, Geborek P, Petersson IF, et al. Predictors of response to methotrexate in early DMARD naive rheumatoid arthritis: results from the initial open-label phase of the SWEFOT trial. Ann Rheum Dis. 2011;70(3):469–75. - PubMed
-
- Bathon JM, Martin RW, Fleischmann RM, Tesser JR, Schiff MH, Keystone EC, et al. A comparison of etanercept and methotrexate in patients with early rheumatoid arthritis. N Engl J Med. 2000;343(22):1586–93. - PubMed
-
- Breedveld FC, Weisman MH, Kavanaugh AF, Cohen SB, Pavelka K, van Vollenhoven R, et al. The PREMIER study: A multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum. 2006;54(1):26–37. - PubMed
-
- Emery P, Breedveld FC, Hall S, Durez P, Chang DJ, Robertson D, et al. Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): a randomised, double-blind, parallel treatment trial. Lancet. 2008;372(9636):375–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
