

Reproducibility of Alzheimer's Disease Cerebrospinal Fluid-Biomarker Measurements under Clinical Routine Conditions
- PMID: 29439341
- PMCID: PMC5817906
- DOI: 10.3233/JAD-170793
Reproducibility of Alzheimer's Disease Cerebrospinal Fluid-Biomarker Measurements under Clinical Routine Conditions
Abstract
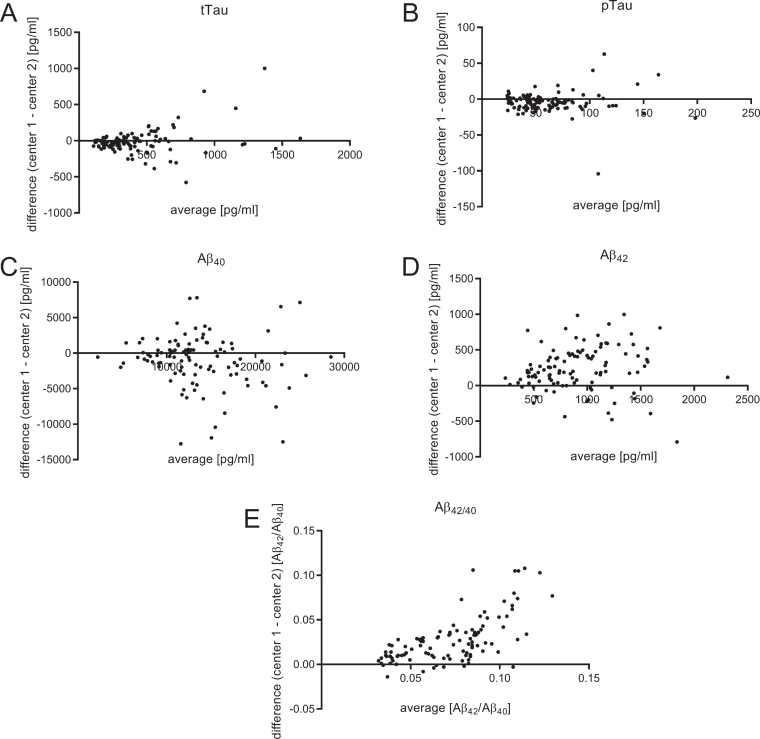
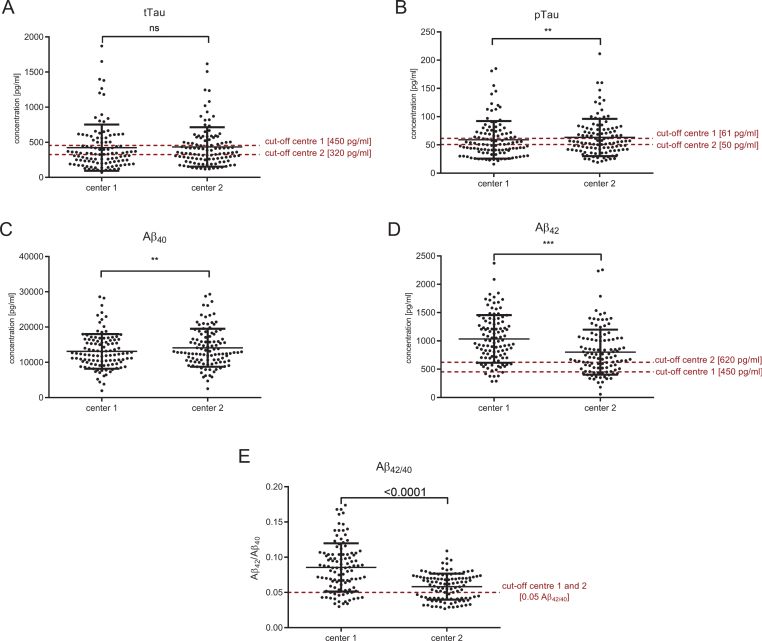
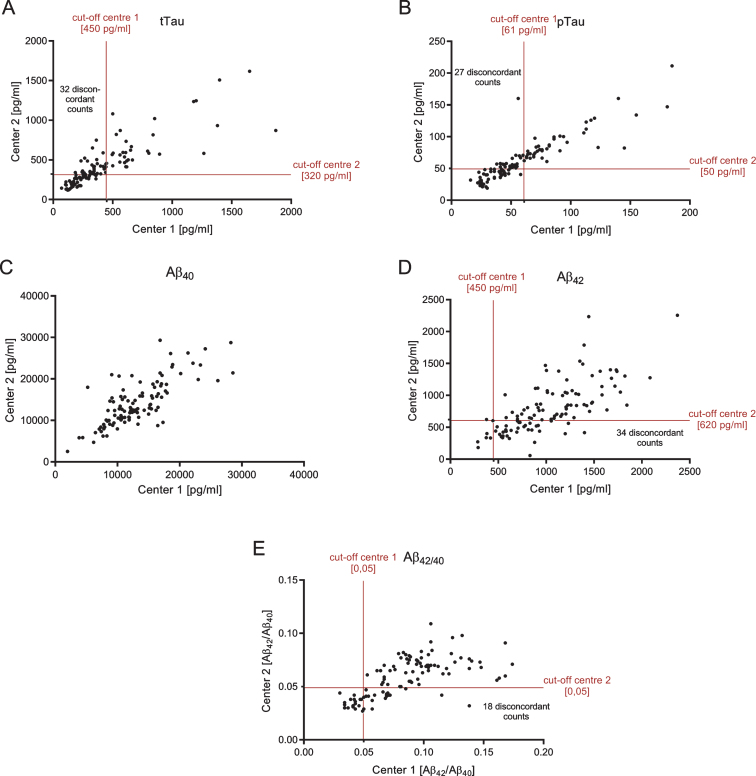
Analysis of cerebrospinal fluid (CSF) is one of the key tools for the state-of-the-art differential diagnosis of dementias. Dementia due to Alzheimer's disease (AD) is characterized by elevated CSF levels of total Tau (tTau) and phospho-181-Tau (pTau) and low CSF amyloid-β42 (Aβ42). Discrepancies in the laboratory analysis of human materials are well known and much effort has been put into harmonization procedures. In this study, we measured CSF biomarkers of more than 100 patients obtained under clinical routine conditions in two different clinical laboratories. The CSF biomarker levels obtained from the two different sites were significantly correlated: R2 = 0.7129 (tTau, p < 0.001), 0.7914 (pTau, p < 0.001), 0.5078 (Aβ42, p < 0.001), 0.5739 (Aβ40, p < 0.001), and 0.4308 (Aβ42/40, p < 0.001). However, the diagnostic classifications of the Aβ42, tTau, and pTau levels of identical subjects into normal versus pathological range made by the two different sites showed substantial discrepancies (31.5%, 29.6%, and 25.0% discordant cases, respectively). Applying Aβ42/40, instead of CSF Aβ42 alone, lead to a reduction of the discordant cases to 16.8%. Our findings suggest that CSF Aβ42/40 can outperform Aβ42 as a biomarker for AD neuropathology, not only under well-controlled study conditions but also in real life clinical routine. Thus, we recommend the inclusion of Aβ42/40 as a CSF biomarker in the diagnostic procedure.
Keywords: Alzheimer’s disease; amyloid-β; biomarker; cerebrospinal fluid; clinical diagnostics.
Figures
References
-
- Cummings JL, Dubois B, Molinuevo JL, Scheltens P (2013) International Work Group Criteria for the diagnosis of Alzheimer disease. Med Clin North Am 97, 363–368. - PubMed
-
- Deuschl G, Maier W (2016) S3-Leitlinie Demenzen. Deutsche Gesellschaft für Neurologie, Hrsg. Leitlinien für Diagnostik und Therapie in der Neurologie, S3-Leitlinie “Demenzen”, http://www.dgn.org/leitlinien, posted 25 January 2016, Accessed 29 November, 2017.
-
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH (2011) The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 263–269. - PMC - PubMed
-
- Sabri O, Sabbagh MN, Seibyl J, Barthel H, Akatsu H, Ouchi Y, Senda K, Murayama S, Ishii K, Takao M, Beach TG, Rowe CC, Leverenz JB, Ghetti B, Ironside JW, Catafau AM, Stephens AW, Mueller A, Koglin N, Hoffmann A, Roth K, Reininger C, Schulz-Schaeffer WJ (2015) Florbetaben PET imaging to detect amyloid beta plaques in Alzheimer’s disease: Phase 3 study. Alzheimers Dement 11, 964–974. - PubMed
-
- Wiltfang J, Esselmann H, Bibl M, Smirnov A, Otto M, Paul S, Schmidt B, Klafki H-W, Maler M, Dyrks T, Bienert M, Beyermann M, Rüther E, Kornhuber J (2002) Highly conserved and disease-specific patterns of carboxyterminally truncated Aβ peptides 1-37/38/39 in addition to 1-40/42 in Alzheimer’s disease and in patients with chronic neuroinflammation. J Neurochem 81, 481–496. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
