

A model to predict disease progression in patients with autosomal dominant polycystic kidney disease (ADPKD): the ADPKD Outcomes Model
- PMID: 29439650
- PMCID: PMC5810027
- DOI: 10.1186/s12882-017-0804-2
A model to predict disease progression in patients with autosomal dominant polycystic kidney disease (ADPKD): the ADPKD Outcomes Model
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is the leading inheritable cause of end-stage renal disease (ESRD); however, the natural course of disease progression is heterogeneous between patients. This study aimed to develop a natural history model of ADPKD that predicted progression rates and long-term outcomes in patients with differing baseline characteristics.
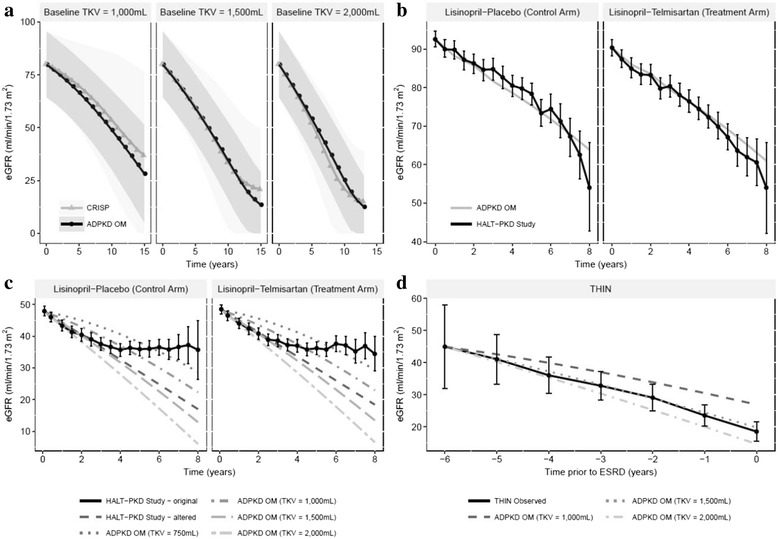
Methods: The ADPKD Outcomes Model (ADPKD-OM) was developed using available patient-level data from the placebo arm of the Tolvaptan Efficacy and Safety in Management of ADPKD and its Outcomes Study (TEMPO 3:4; ClinicalTrials.gov identifier NCT00428948). Multivariable regression equations estimating annual rates of ADPKD progression, in terms of total kidney volume (TKV) and estimated glomerular filtration rate, formed the basis of the lifetime patient-level simulation model. Outputs of the ADPKD-OM were compared against external data sources to validate model accuracy and generalisability to other ADPKD patient populations, then used to predict long-term outcomes in a cohort matched to the overall TEMPO 3:4 study population.
Results: A cohort with baseline patient characteristics consistent with TEMPO 3:4 was predicted to reach ESRD at a mean age of 52 years. Most patients (85%) were predicted to reach ESRD by the age of 65 years, with many progressing to ESRD earlier in life (18, 36 and 56% by the age of 45, 50 and 55 years, respectively). Consistent with previous research and clinical opinion, analyses supported the selection of baseline TKV as a prognostic factor for ADPKD progression, and demonstrated its value as a strong predictor of future ESRD risk. Validation exercises and illustrative analyses confirmed the ability of the ADPKD-OM to accurately predict disease progression towards ESRD across a range of clinically-relevant patient profiles.
Conclusions: The ADPKD-OM represents a robust tool to predict natural disease progression and long-term outcomes in ADPKD patients, based on readily available and/or measurable clinical characteristics. In conjunction with clinical judgement, it has the potential to support decision-making in research and clinical practice.
Keywords: Disease modelling; ESRD; End-stage renal disease; Kidney volume; Renal function decline; Renal progression.
Conflict of interest statement
Ethics approval and consent to participate
This article is based on previously conducted research, and does not involve any new studies of human or animal subjects performed by any of the authors.
Consent for publication
Not applicable.
Competing interests
ACMO, BØ, RS, FS, M-CVC, and GW have received honoraria from Otsuka Pharmaceutical Europe Ltd. for serving on advisory board meetings and/or lectures. PM and HBW are employees of HEOR Ltd., a company sponsored by Otsuka Pharmaceutical Europe Ltd. to build the model. KO and PR are employees of Otsuka Pharmaceutical Europe Ltd.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
-
- Spithoven EM, Kramer A, Meijer E, Orskov B, Wanner C, Abad JM, et al. Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival—an analysis of data from the ERA-EDTA registry. Nephrol Dial Transplant. 2014;29(Suppl 4):iv15–iv25. doi: 10.1093/ndt/gfu017. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
