

Stereotactic Body Radiotherapy (SBRT) for liver metastasis - clinical outcomes from the international multi-institutional RSSearch® Patient Registry
- PMID: 29439707
- PMCID: PMC5811977
- DOI: 10.1186/s13014-018-0969-2
Stereotactic Body Radiotherapy (SBRT) for liver metastasis - clinical outcomes from the international multi-institutional RSSearch® Patient Registry
Abstract
Background: Stereotactic body radiotherapy (SBRT) is an emerging treatment option for liver metastases in patients unsuitable for surgery. We investigated factors associated with clinical outcomes for liver metastases treated with SBRT from a multi-center, international patient registry.
Methods: Patients with liver metastases treated with SBRT were identified in the RSSearch® Patient Registry. Patient, tumor and treatment characteristics associated with treatment outcomes were assessed. Dose fractionations were normalized to BED10. Overall survival (OS) and local control (LC) were evaluated using Kaplan Meier analysis and log-rank test.
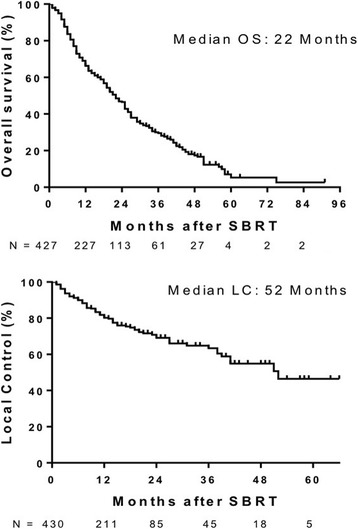
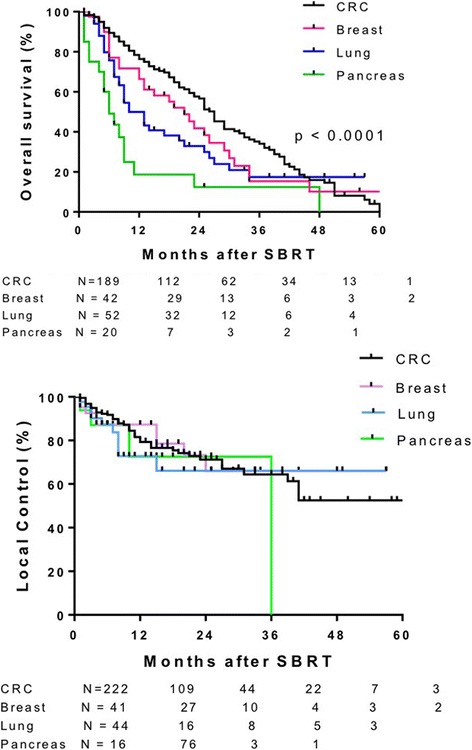
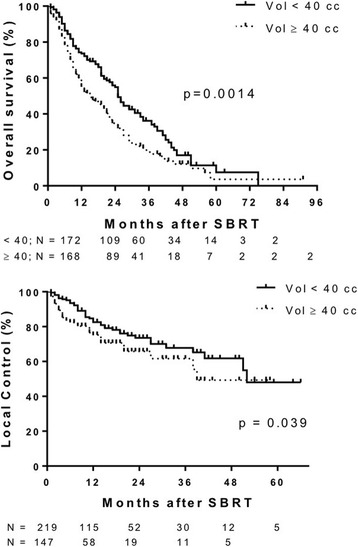
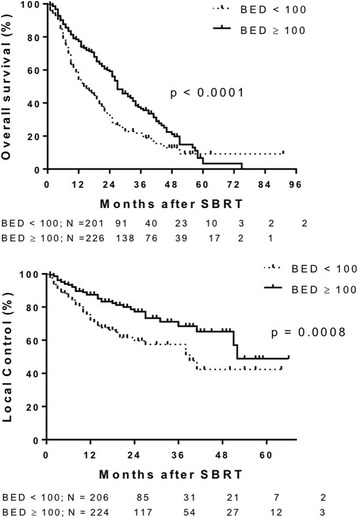
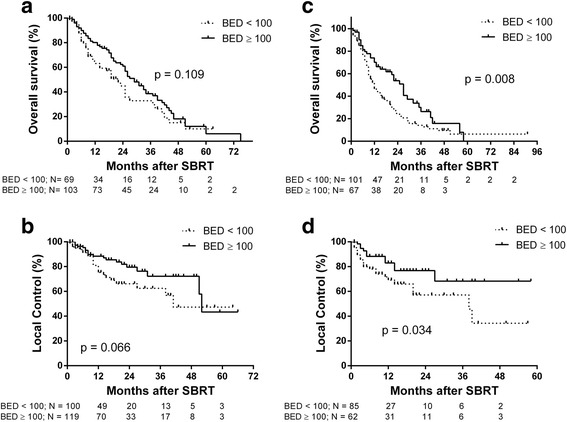
Results: The study included 427 patients with 568 liver metastases from 25 academic and community-based centers. Median age was 67 years (31-91 years). Colorectal adenocarcinoma (CRC) was the most common primary cancer. 73% of patients received prior chemotherapy. Median tumor volume was 40 cm3 (1.6-877 cm3), median SBRT dose was 45 Gy (12-60 Gy) delivered in a median of 3 fractions [1-5]. At a median follow-up of 14 months (1-91 months) the median overall survival (OS) was 22 months. Median OS was greater for patients with CRC (27 mo), breast (21 mo) and gynecological (25 mo) metastases compared to lung (10 mo), other gastro-intestinal (GI) (18 mo) and pancreatic (6 mo) primaries (p < 0.0001). Smaller tumor volumes (< 40 cm3) correlated with improved OS (25 months vs 15 months p = 0.0014). BED10 ≥ 100 Gy was also associated with improved OS (27 months vs 15 months p < 0.0001). Local control (LC) was evaluable in 430 liver metastases from 324 patients. Two-year LC rates was better for BED10 ≥ 100 Gy (77.2% vs 59.6%) and the median LC was better for tumors < 40 cm3 (52 vs 39 months). There was no difference in LC based on histology of the primary tumor.
Conclusions: In a large, multi-institutional series of patients with liver metastasis treated with SBRT, reasonable LC and OS was observed. OS and LC depended on dose and tumor volume, while OS varied by primary tumor. Future prospective trials on the role of SBRT for liver metastasis from different primaries in the setting of multidisciplinary management including systemic therapy, is warranted.
Trial registration: Clinicaltrials.gov: NCT01885299 .
Keywords: Liver metastasis; RSSearch registry; SBRT.
Conflict of interest statement
Ethics approval and consent to participate
All participating institutions were required to have Institutional Review Board/Ethics Committee approval prior to entering patients into the registry.
All subjects were required to sign an informed consent specific for entry into the registry.
Consent for publication
Patient informed consent included consent for publication. All investigators provided consent for publication.
Competing interests
The authors do not have competing interest in the publication of this cumulative data.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
