

The Treatment of Temporomandibular Joint Dislocation
- PMID: 29439762
- PMCID: PMC5817180
- DOI: 10.3238/arztebl.2018.0059
The Treatment of Temporomandibular Joint Dislocation
Abstract
Background: The estimated incidence of temporomandibular joint dislocation in Germany is at least 25/100 000 per year. A correct diagnosis and the initiation of appropriate treatment without delay are essential if permanent damage to the joint is to be avoided.
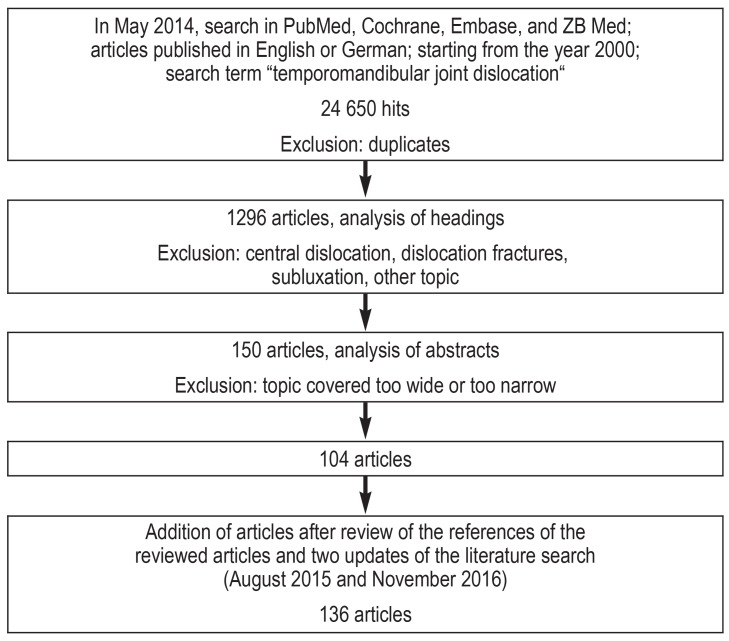
Methods: This review is based on pertinent publications retrieved by a systematic search in the PubMed, Cochrane, Embase, and ZB Med databases.
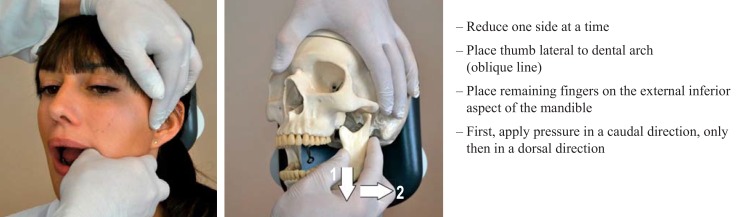
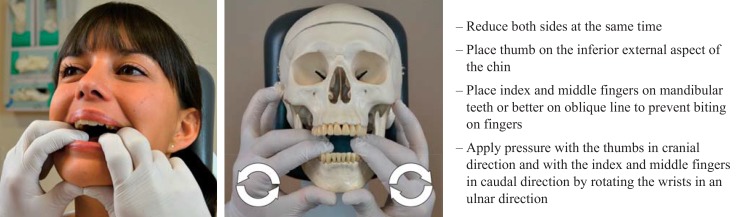
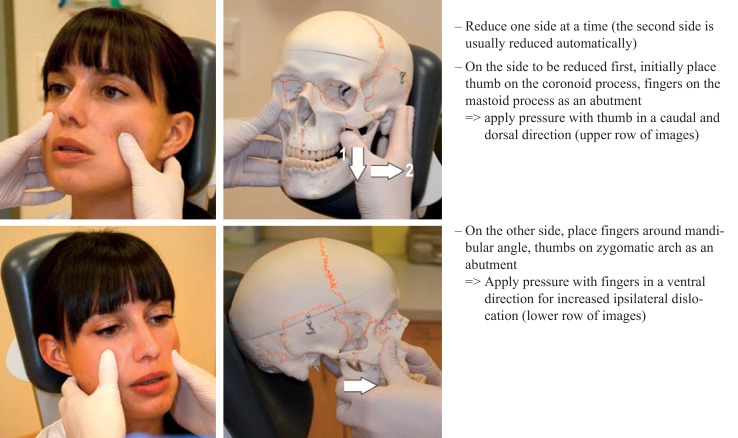
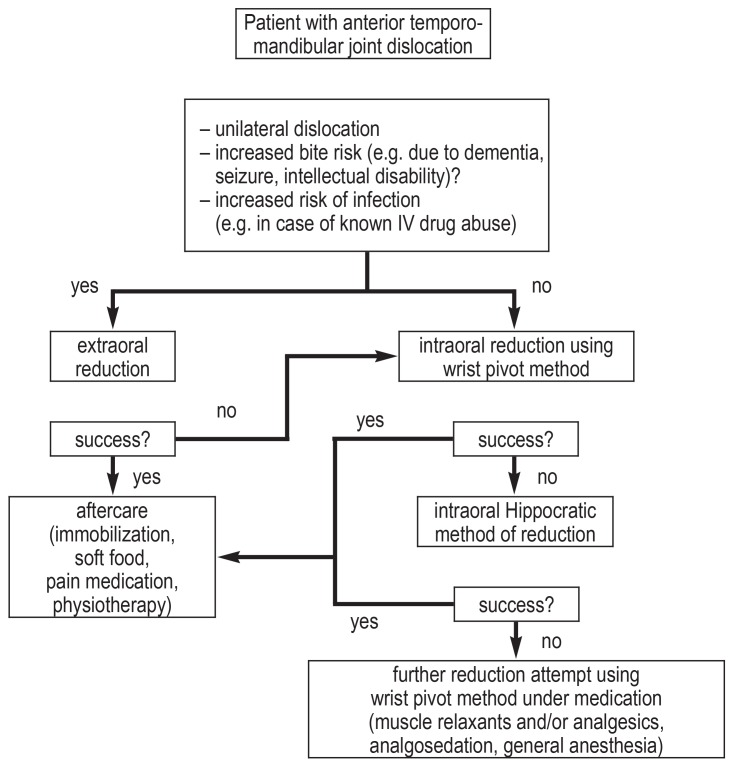
Results: The initial search yielded 24 650 hits; duplicates were removed and 136 studies were chosen for further analysis. The diagnosis of temporomandibular joint dislocation is generally made clinically from the finding of a lower jaw that is fixed in the open position. Acute dislocations are manually repositioned at once. The most common method is Hippocratic repositioning, in which the physician's thumb is placed laterally next to the teeth and the other fingers are placed on the lower surface of the lower jaw. The physician then exerts pressure, first caudally, then dorsally. Repositioning is carried out in two steps. For dislocations that have been present for a longer time, manual repositioning may be ineffective and surgery may be needed. Recurrent dislocation can be treated in a minimally invasive way with botulinum toxin injections or autologous blood therapy. Surgery may be needed if these methods are ineffective.
Conclusion: There have been no more than a few randomized, controlled trials of treatments for temporomandibular joint dislocation, in particular concerning minimally invasive and open surgical treatments, and therefore only limited evidence-based conclusions can be drawn. Nonetheless, the diagnostic and therapeutic standards that have been established in recent years have gained wide international acceptance.
Figures

References
-
- Sang LK, Mulupi E, Akama MK, Muriithi JM, Macigo FG, Chindia ML. Temporomandibular joint dislocation in Nairobi. East Afr Med J. 2010;87:32–37. - PubMed
-
- Ugboko VI, Oginni FO, Ajike SO, Olasoji HO, Adebayo ET. A survey of temporomandibular joint dislocation: aetiology, demographics, risk factors and management in 96 Nigerian cases. Int J Oral Maxillofac Surg. 2005;34:499–502. - PubMed
-
- Forshaw R. Reduction of temporomandibular joint dislocation: an ancient technique that has stood the test of time. Br Dent J. 2015;218:691–693. - PubMed
-
- Momani M, Abdallah MN, Al-Sebaie D, Tamimi F. Rehabilitation of a completely edentulous patient with nonreducible bilateral anterior dislocation of the temporomandibular joint: a prosthodontic challenge-clinical report. J Prosthodont. 2015;25:402–406. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical