

Nomogram for predicting radiation maculopathy in patients treated with Ruthenium-106 plaque brachytherapy for uveal melanoma
- PMID: 29441098
- PMCID: PMC5807992
- DOI: 10.5114/jcb.2017.71795
Nomogram for predicting radiation maculopathy in patients treated with Ruthenium-106 plaque brachytherapy for uveal melanoma
Abstract
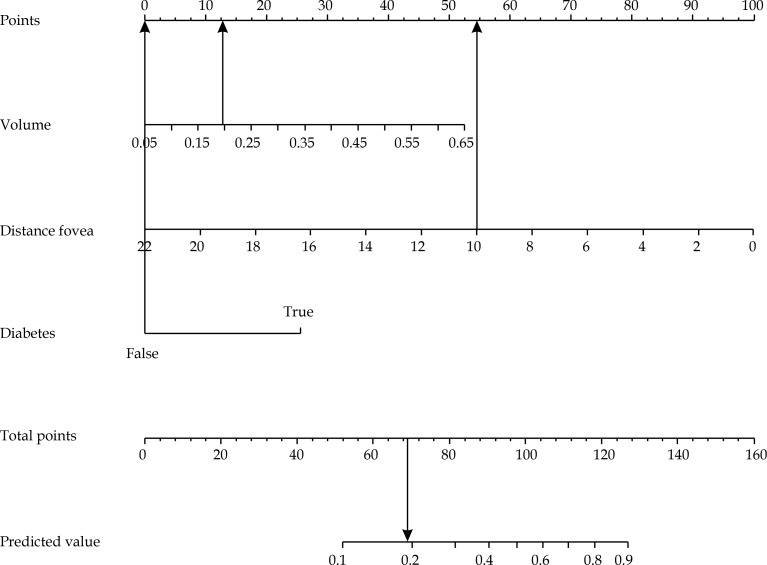
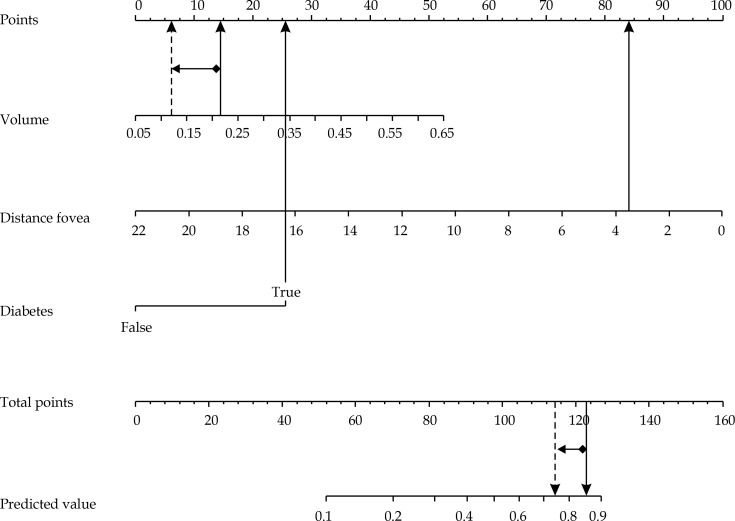
Purpose: To develop a predictive model and nomogram for maculopathy occurrence at 3 years after 106Ru/106Rh plaque brachytherapy in uveal melanoma.
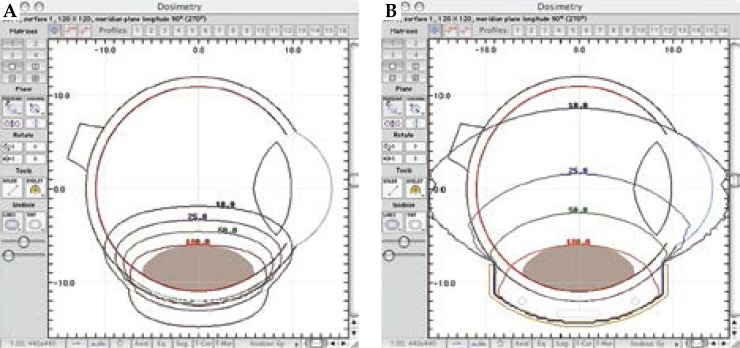
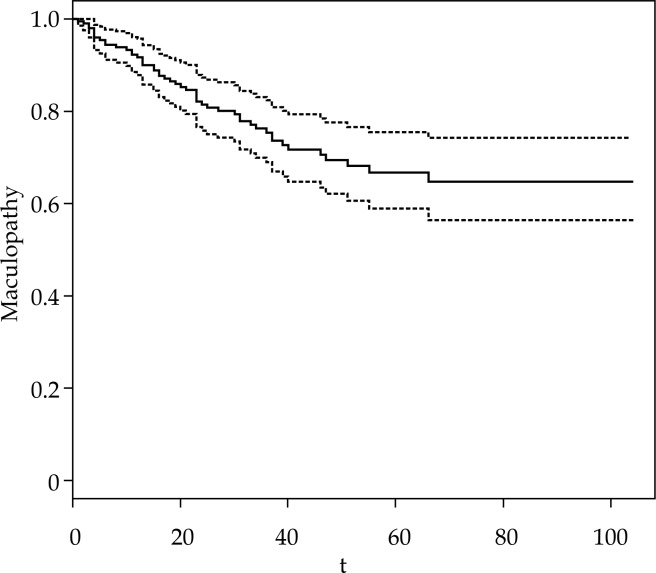
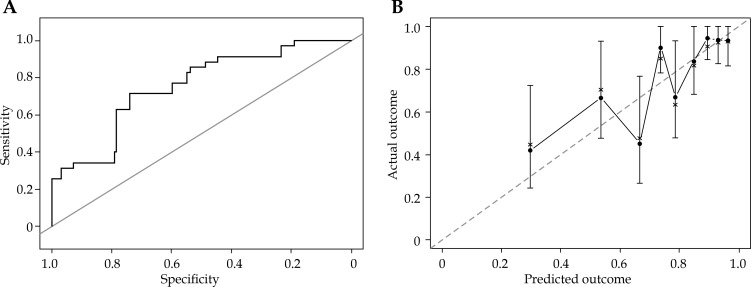
Material and methods: Clinical records of patients affected by choroidal melanoma and treated with 106Ru/106Rh plaque from December 2006 to December 2014 were retrospectively reviewed. Inclusion criteria were: dome-shaped melanoma, distance to the fovea > 1.5 mm, tumor thickness > 2 mm, and follow-up > 4 months. The delivered dose to the tumor apex was 100 Gy. Primary endpoint of this investigation was the occurrence of radiation maculopathy at 3 years. Analyzed factors were as follows: gender, age, diabetes, tumor size (volume, area, largest basal diameter and apical height), type of plaque, distance to the fovea, presence of exudative detachment, drusen, orange pigment, radiation dose to the fovea and sclera. Univariate and multivariate Cox proportional hazards analyses were used to define the impact of baseline patient factors on the occurrence of maculopathy. Kaplan-Meier curves were used to estimate freedom from the occurrence of the maculopathy. The model performance was evaluated through internal validation using area under the ROC curve (AUC), and calibration with Gronnesby and Borgan tests.
Results: One hundred ninety-seven patients were considered for the final analysis. Radiation-related maculopathy at 3 years was observed in 41 patients. The proposed nomogram can predict maculopathy at 3 years with an AUC of 0.75. Distance to fovea appeared to be the main prognostic factor of the predictive model (hazard ratio of 0.83 [0.76-0.90], p < 0.01). Diabetes (hazard radio of 2.92 [1.38-6.20], p < 0.01), and tumor volume (hazard radio of 21.6 [1.66-281.14], p = 0.02) were significantly predictive for maculopathy occurrence. The calibration showed no statistical difference between actual and predicted maculopathy (p = 1).
Conclusions: Our predictive model, together with its nomogram, could be a useful tool to predict the occurrence of radiation maculopathy at 3 years after the treatment.
Keywords: brachytherapy; maculopathy; nomogram; radiotherapy; ruthenium plaque; uveal melanoma.
Figures
References
-
- Singh AD, Topham A. Incidence of uveal melanoma in the United States: 1973-1997. Ophthalmology. 2003;110:956–961. - PubMed
-
- Diener-West M, Earle JD, Fine SL, et al. Collaborative Ocular Melanoma Study Group The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma, III: initial mortality findings. COMS Report No. 18. Arch Ophthalmol. 2001;119:969–982. - PubMed
-
- Diener-West M, Hawkins BS, Markowitz JA, et al. A review of mortality from choroidal melanoma. II. A meta-analysis of 5-year mortality rates following enucleation, 1966 through 1988. Arch Ophthalmol. 1992;110:245–250. - PubMed
-
- Seddon JM, Gragoudas ES, Egan KM, et al. Relative survival rates after alternative therapies for uveal melanoma. Ophthalmology. 1990;97:769–777. - PubMed
-
- Augsburger JJ, Schneider S, Freire J, et al. Survival following enucleation versus plaque radiotherapy in statistically matched subgroups of patients with choroidal melanomas: results in patients treated between 1980 and 1987. Graefes Arch Clin Exp Ophthalmol. 1999;237:558–567. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous