Is vaginal reflux associated with urinary tract infection in female children under the age of 36 months?
- PMID: 29441108
- PMCID: PMC5807986
- DOI: 10.3345/kjp.2018.61.1.17
Is vaginal reflux associated with urinary tract infection in female children under the age of 36 months?
Abstract
Purpose: To determine the relationship between vaginal reflux (VR) and urinary tract infection (UTI) in female children aged <36 months.
Methods: A single center retrospective study was performed for 191 girls aged <36 months, with a diagnosis of febrile UTI, who underwent a voiding cystourethrography (VCUG) for assessment of vesicoureteral reflux (VUR) at Sanggye Paik Hospital. Fifty-one girls, who underwent VCUG for assessment of congenital hydronephrosis or renal pelvis dilatation, without a UTI, formed the control group. The correlation between the presence and grade of VR and UTI was evaluated.
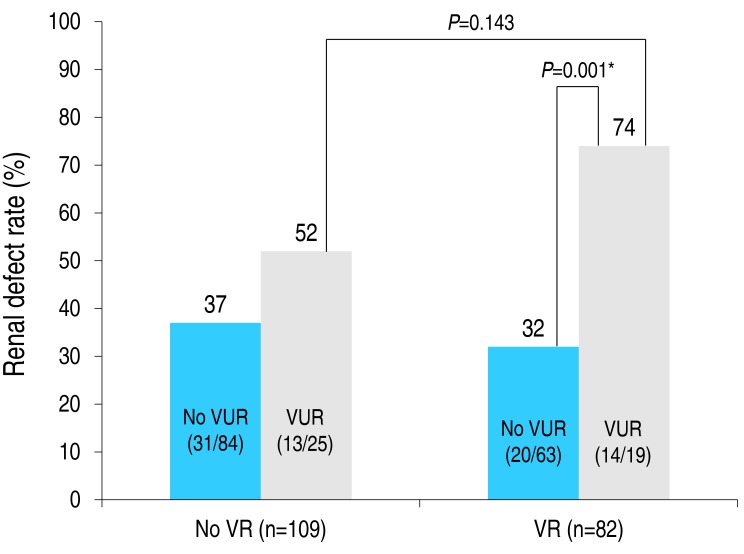
Results: The prevalence rate of VR was higher in the UTI (42.9%) than control (13.7%) group (P<0.05), with a higher VR severity grade in the UTI (mean, 0.64) than control (mean, 0.18) group (P<0.05). On subanalysis with age-matching (UTI group: n=126, age, 5.28±2.13 months; control group: n=22, age, 4.79±2.40 months; P=0.33), both VR prevalence (43.65% vs. 18.18%, P<0.05) and grade (0.65 vs. 0.22, P<0.05) remained higher in the UTI than control group. Presence and higher grade of VR were associated with UTI recurrence (P<0.05). VR was correlated to urosepsis (P<0.05). The renal defect rate of patients with VR (VR [+]/VUR [+]) was not different from that of patients without VR (74% vs. 52%, P=0.143) in the VUR group; however, it was higher than that of VR (+)/VUR (-) patients (74% vs. 32%, P=0.001). If a child with VR (+)/VUR (+) is exposed to a UTI, the risk of renal defect increases.
Conclusion: Occurrence of VR is associated with UTI recurrence and urosepsis in pediatric female patients.
Keywords: Urinary tract infection, Vesicoureteral reflux; Vaginal reflux.
Conflict of interest statement
Conflicts of interest: No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Elder JS. Urinary tract infection. In: Kliegman RM, Stanton BF, St. Geme JW III, Schor NF, Behrman RE, editors. Nelson textbook of pediatrics. 20th ed. Philadelphia: Elsevier Saunders; 2011. pp. 2558–2559.
-
- Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA. 2007;298:179–186. - PubMed
-
- Montini G, Tullus K, Hewitt I. Febrile urinary tract infections in children. N Engl J Med. 2011;365:239–250. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources