

Complications in tube thoracostomy: Systematic review and meta-analysis
- PMID: 29443856
- PMCID: PMC6081248
- DOI: 10.1097/TA.0000000000001840
Complications in tube thoracostomy: Systematic review and meta-analysis
Abstract
Background: Tube thoracostomy (TT) complications and their reported rates are highly variable (1-40%) and inconsistently classified. Consistent TT complication classification must be applied to compare reported literature to standardize TT placement. We aim to determine the overall TT-related complication rates in patients receiving TT for traumatic indications using uniform definitions.
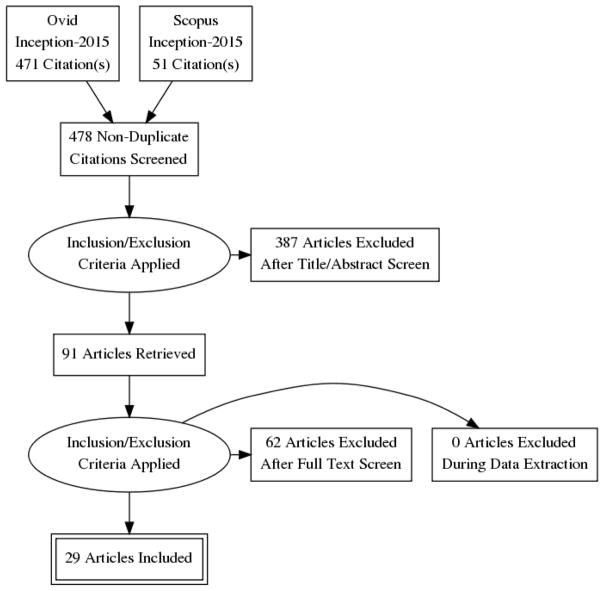
Methods: Systematic review and meta-analysis was performed assessing TT-related complications. Comprehensive search of several databases (1975-2015) was conducted. We included studies that reported on bedside TT insertion (≥22 Fr) in trauma patients. Data were abstracted from eligible articles by independent reviewers with discrepancies reconciled by a third. Analyses were based on complication category subtypes: insertional, positional, removal, infection/immunologic/education, and malfunction.
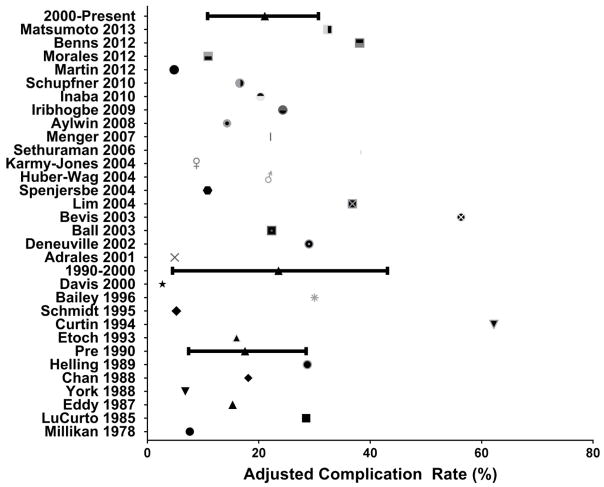
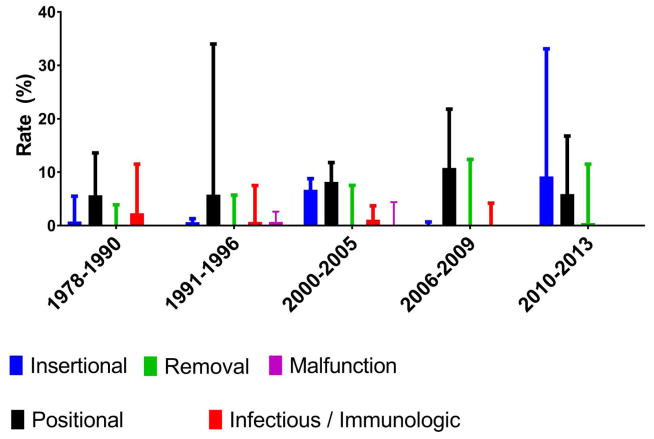
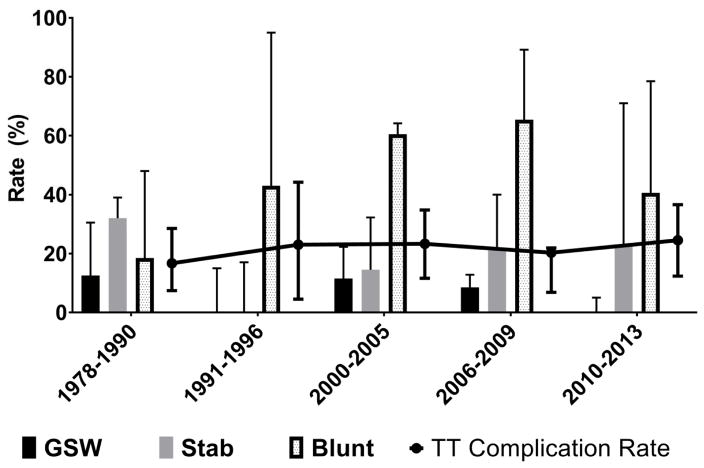
Results: Database search resulted in 478 studies; after applying criteria 29 studies were analyzed representing 4,981 TTs. Injury mechanisms included blunt 60% (49-71), stab 27% (17-34), and gunshot 13% (7.8-10). Overall, median complication rate was 19% (95% confidence interval, 14-24.3). Complication subtypes included insertional (15.3%), positional (53.1%), removal (16.2%), infection/immunologic (14.8%), and malfunction (0.6%). Complication rates did not change significantly over time for insertional, immunologic, or removal p = 0.8. Over time, there was a decrease in infectious TT-related complications as well as an increase in positional TT complications.
Conclusion: Generation of evidence-based approaches to improve TT insertion outcomes is difficult because a variety of complication classifications has been used. This meta-analysis of complications after TT insertion in trauma patients suggests that complications have not changed over time remaining stable at 19% over the past three decades.
Level of evidence: Systematic review and meta-analysis, level III.
Figures
References
-
- Hernandez MC, Zeb MH, Heller SF, Zielinski MD, Aho JM. Tube Thoracostomy Complications Increase Cost. World J Surg. 2017;41(6):1482–1487. - PubMed
-
- Chan L, Reilly KM, Henderson C, Kahn F, Salluzzo RF. Complication rates of tube thoracostomy. Am J Emerg Med. 1997;15(4):368–70.7. - PubMed
-
- Millikan JS, Moore EE, Steiner E, Aragon GE, Van Way CW., 3rd Complications of tube thoracostomy for acute trauma. Am J Surg. 1980;140(6):738–41. - PubMed
-
- LoCurto JJ, Jr, Tischler CD, Swan KG, Rocko JM, Blackwood JM, Griffin CC, Lazaro EJ, Reiner DS. Tube thoracostomy and trauma--antibiotics or not? J Trauma. 1986;26(12):1067–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
