

Comparison of Strategies and Incidence Thresholds for Vi Conjugate Vaccines Against Typhoid Fever: A Cost-effectiveness Modeling Study
- PMID: 29444257
- PMCID: PMC6226717
- DOI: 10.1093/infdis/jix598
Comparison of Strategies and Incidence Thresholds for Vi Conjugate Vaccines Against Typhoid Fever: A Cost-effectiveness Modeling Study
Abstract
Background: Typhoid fever remains a major public health problem globally. While new Vi conjugate vaccines hold promise for averting disease, the optimal programmatic delivery remains unclear. We aimed to identify the strategies and associated epidemiologic conditions under which Vi conjugate vaccines would be cost-effective.
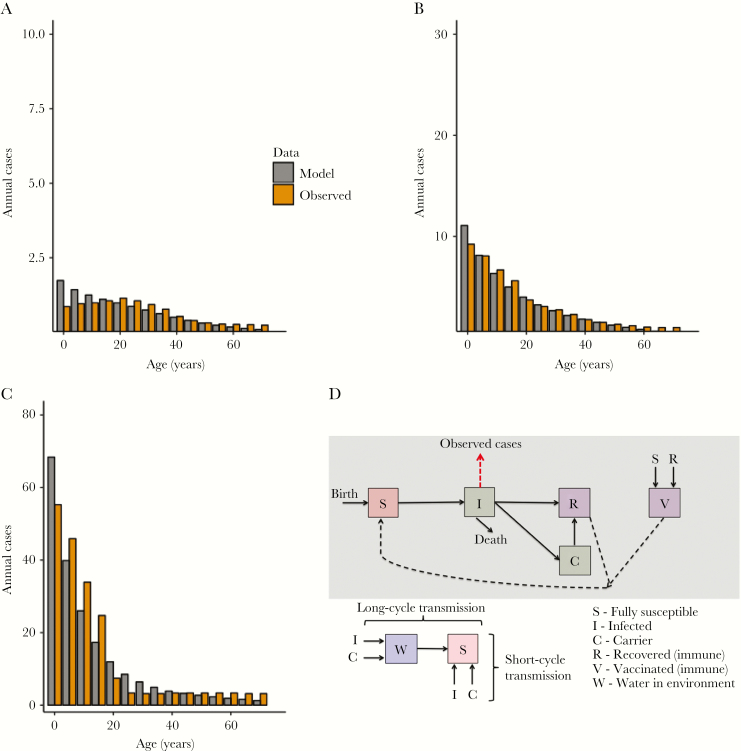
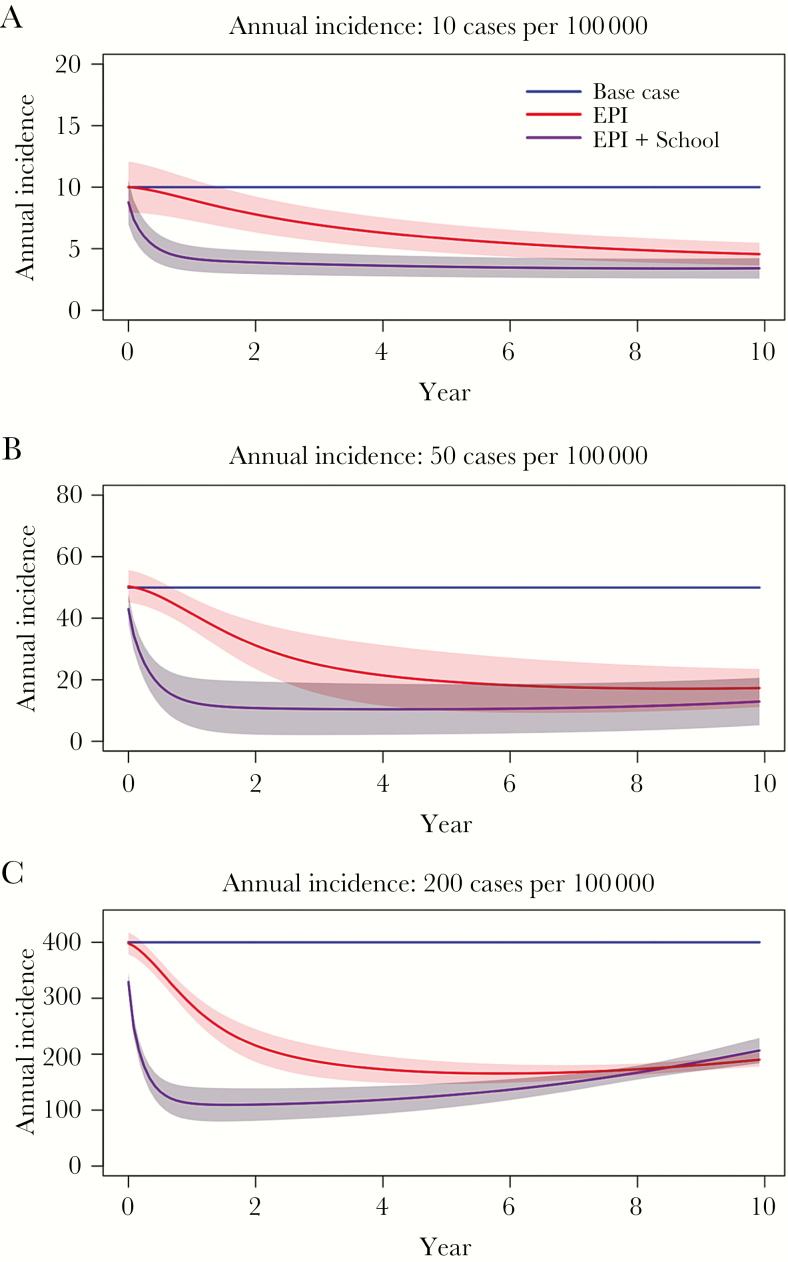
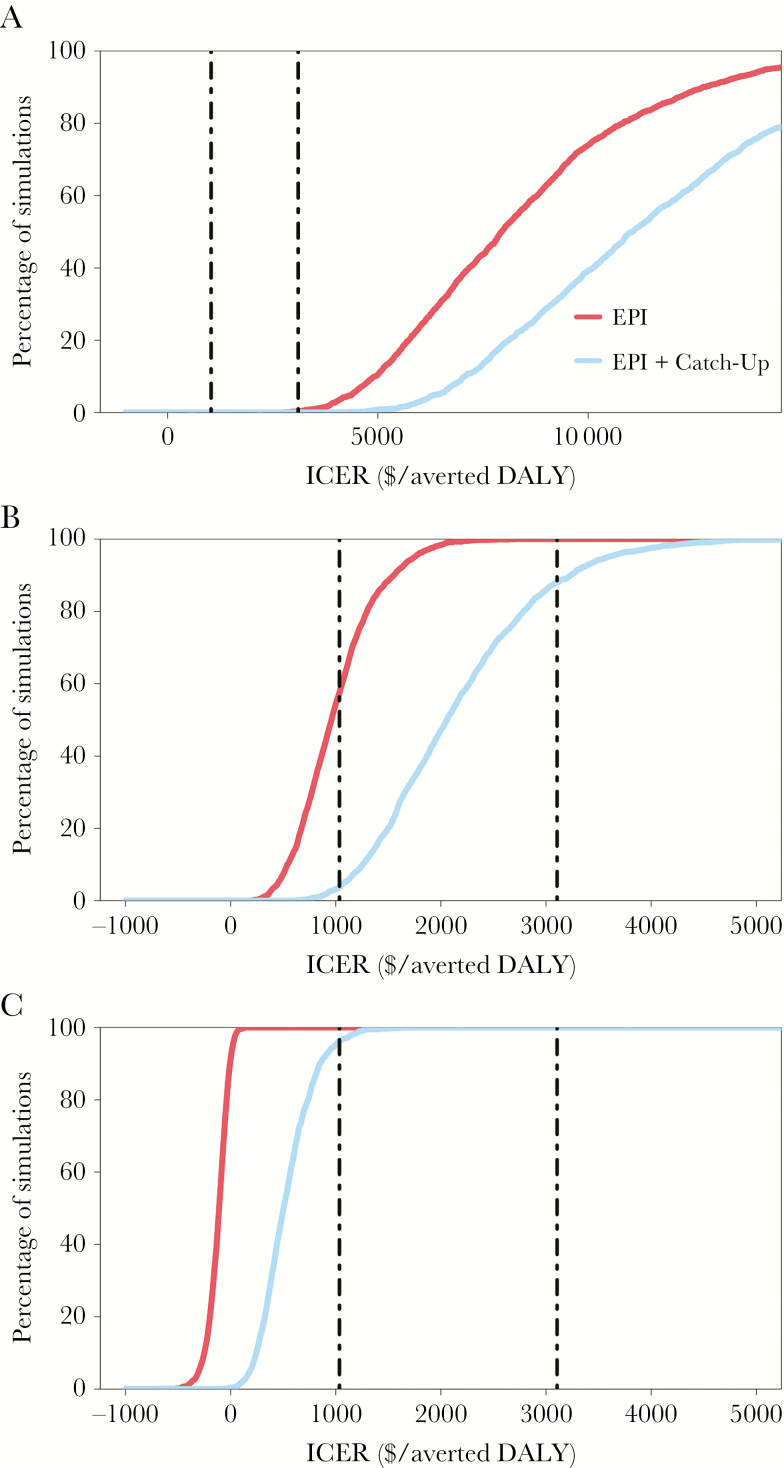
Methods: We developed a dynamic, age-structured transmission and cost-effectiveness model that simulated multiple vaccination strategies with a typhoid Vi conjugate vaccine from a societal perspective. We simulated 10-year vaccination programs with (1) routine immunization of infants (aged <1 year) through the Expanded Program on Immunization (EPI) and (2) routine immunization of infants through the EPI plus a 1-time catch-up campaign in school-aged children (aged 5-14 years). In the base case analysis, we assumed a 0.5% case-fatality rate for all cases of clinically symptomatic typhoid fever and defined strategies as highly cost-effective by using the definition of a low-income country (defined as a country with a gross domestic product of $1045 per capita). We defined incidence as the true number of clinically symptomatic people in the population per year.
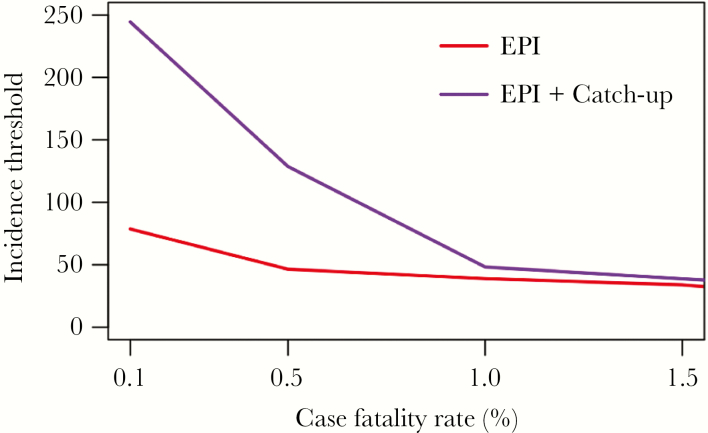
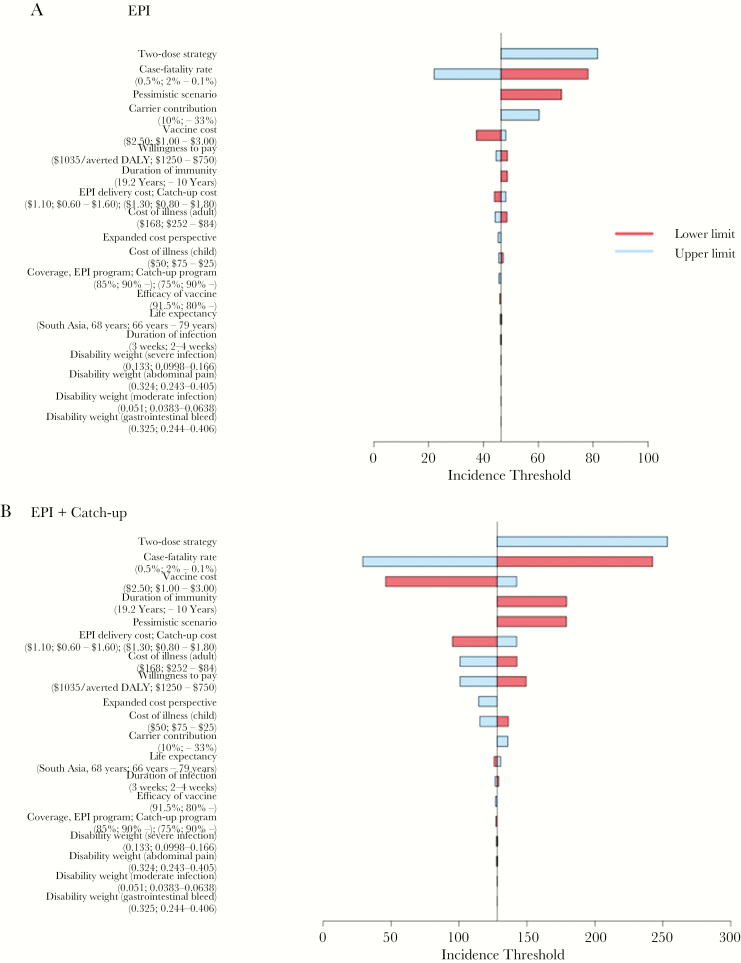
Results: Vi conjugate typhoid vaccines were highly cost-effective when administered by routine immunization activities through the EPI in settings with an annual incidence of >50 cases/100000 (95% uncertainty interval, 40-75 cases) and when administered through the EPI plus a catch-up campaign in settings with an annual incidence of >130 cases/100000 (95% uncertainty interval, 50-395 cases). The incidence threshold was sensitive to the typhoid-related case-fatality rate, carrier contribution to transmission, vaccine characteristics, and country-specific economic threshold for cost-effectiveness.
Conclusions: Typhoid Vi conjugate vaccines would be highly cost-effective in low-income countries in settings of moderate typhoid incidence (50 cases/100000 annually). These results were sensitive to case-fatality rates, underscoring the need to consider factors contributing to typhoid mortality (eg, healthcare access and antimicrobial resistance) in the global vaccination strategy.
Figures
References
-
- Mogasale V, Maskery B, Ochiai RL et al. . Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Glob Health 2014; 2:e570–80. - PubMed
-
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386:743–800. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
