

Serum IgG subclass levels and risk of exacerbations and hospitalizations in patients with COPD
- PMID: 29444682
- PMCID: PMC5813358
- DOI: 10.1186/s12931-018-0733-z
Serum IgG subclass levels and risk of exacerbations and hospitalizations in patients with COPD
Abstract
Background: The literature is scarce regarding the prevalence and clinical impact of IgG subclass deficiency in COPD. We investigated the prevalence of IgG subclass deficiencies and their association with exacerbations and hospitalizations using subjects from two COPD cohorts.
Methods: We measured IgG subclass levels using immunonephelometry in serum samples from participants enrolled in two previous COPD trials: Macrolide Azithromycin for Prevention of Exacerbations of COPD (MACRO; n = 976) and Simvastatin for the Prevention of Exacerbations in Moderate-to-Severe COPD (STATCOPE; n = 653). All samples were collected from clinically stable participants upon entry into both studies. IgG subclass deficiency was diagnosed when IgG subclass levels were below their respective lower limit of normal: IgG1 < 2.8 g/L; IgG2 < 1.15 g/L; IgG3 < 0.24 g/L; and IgG4 < 0.052 g/L. To investigate the impact of IgG subclass levels on time to first exacerbation or hospitalization, we log-transformed IgG levels and performed Cox regression models, with adjustments for confounders.
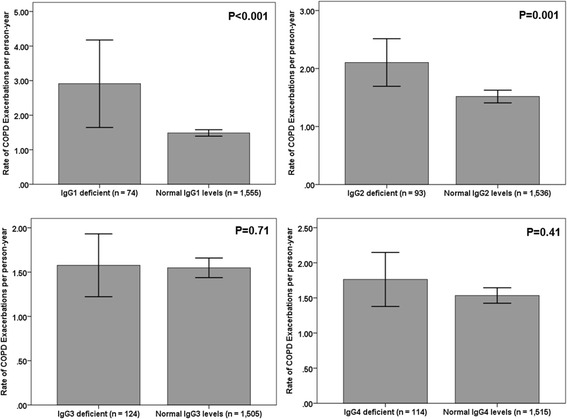
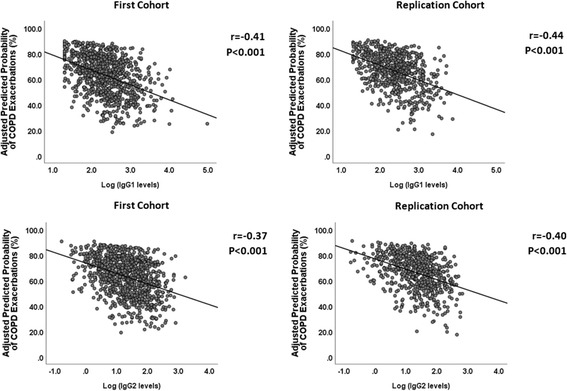
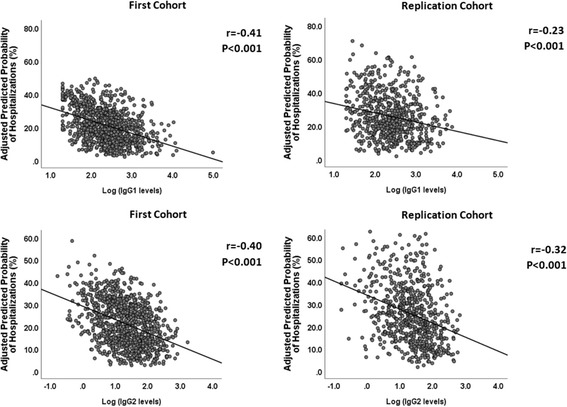
Results: One or more IgG subclass deficiencies were found in 173 (17.7%) and 133 (20.4%) participants in MACRO and STATCOPE, respectively. Lower IgG1 or IgG2 levels resulted in increased risk of exacerbations with adjusted hazard ratios (HR) of 1.30 (95% CI, 1.10-1.54, p < 0.01) and 1.19 (95% CI, 1.05-1.35, p < 0.01), respectively in the MACRO study, with STATCOPE yielding similar results. Reduced IgG1 or IgG2 levels were also associated with increased risk of hospitalizations: the adjusted HR for IgG1 and IgG2 was 1.52 (95% CI: 1.15-2.02, p < 0.01) and 1.33 (95% CI, 1.08-1.64, p < 0.01), respectively for the MACRO study; in STATCOPE, only IgG2 was an independent predictor of hospitalization. In our multivariate Cox models, IgG3 and IgG4 levels did not result in significant associations for both outcomes in either MACRO or STATCOPE cohorts.
Conclusions: Approximately 1 in 5 COPD patients had one or more IgG subclass deficiencies. Reduced IgG subclass levels were independent risk factors for both COPD exacerbations (IgG1 and IgG2) and hospitalizations (IgG2) in two COPD cohorts.
Trial registration: This study used serum samples from participants of the MACRO ( NCT00325897 ) and STATCOPE ( NCT01061671 ) trials.
Keywords: COPD; Exacerbation; Hospitalization; IgG; IgG subclass deficiency.
Conflict of interest statement
Ethics approval and consent to participate
Both trials received approval from each participating institutions’ local research ethics board. This analysis received approval from the University of British Columbia/Providence Health Care Research Ethics Committee (Approval No. H16–03232).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017;195(5):557–582. doi: 10.1164/rccm.201701-0218PP. - DOI - PubMed
-
- Umetsu DT, Ambrosino DM, Quinti I, Siber GR, Geha RS. Recurrent sinopulmonary infection and impaired antibody response to bacterial capsular polysaccharide antigen in children with selective IgG-subclass deficiency. N. Engl. J. Med. 1985;313(20):1247–1251. doi: 10.1056/NEJM198511143132002. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
