

Analysis of airway pathology in COPD using a combination of computed tomography, micro-computed tomography and histology
- PMID: 29444912
- PMCID: PMC6691959
- DOI: 10.1183/13993003.01245-2017
Analysis of airway pathology in COPD using a combination of computed tomography, micro-computed tomography and histology
Abstract
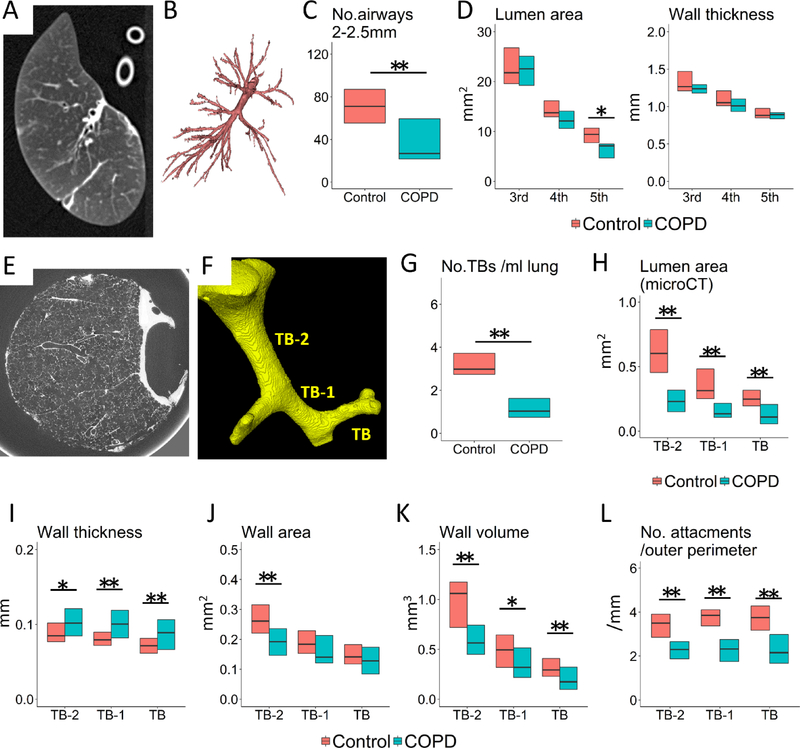
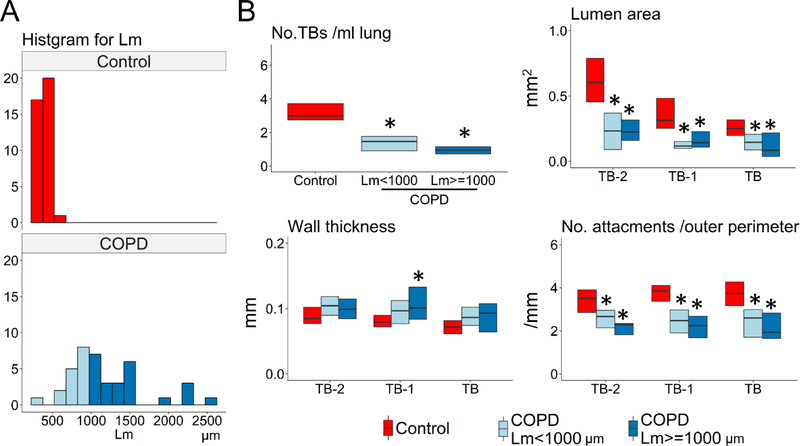
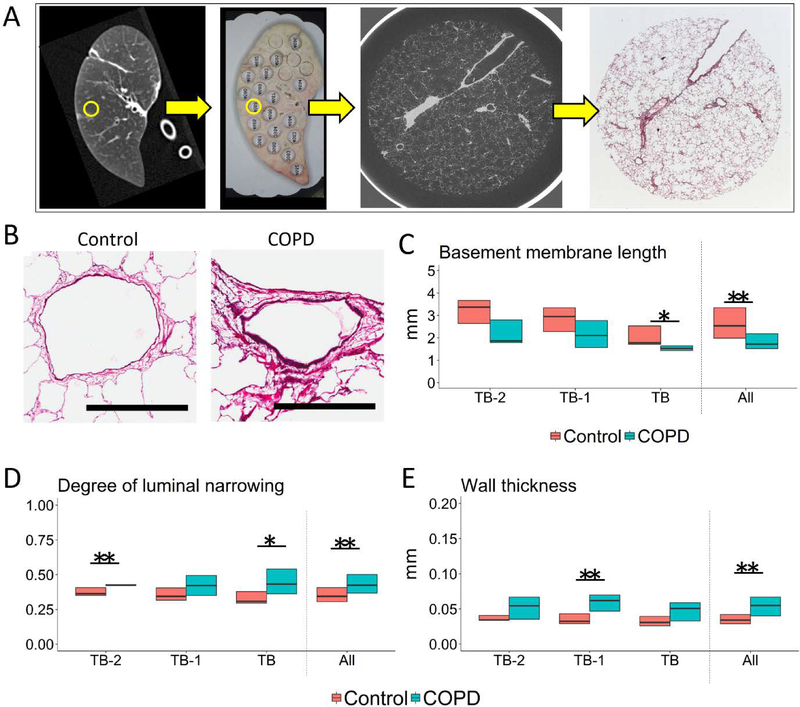
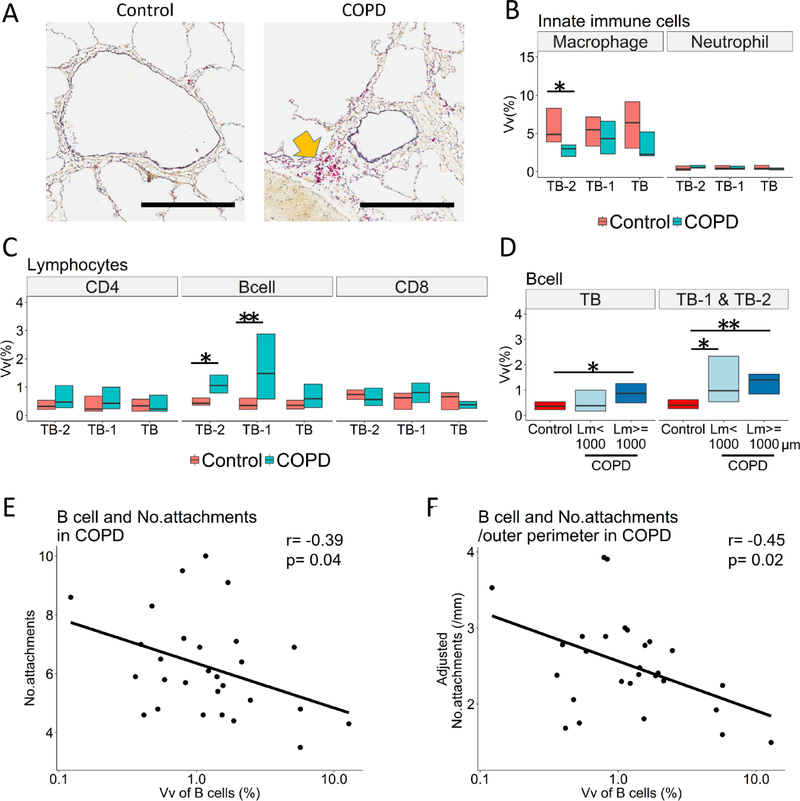
The small conducting airways are the major site of obstruction in chronic obstructive pulmonary disease (COPD). This study examined small airway pathology using a novel combination of multidetector row computed tomography (MDCT), micro-computed tomography (microCT) and histology.Airway branches visible on specimen MDCT were counted and the dimensions of the third- to fifth-generation airways were computed, while the terminal bronchioles (designated TB), preterminal bronchioles (TB-1) and pre-preterminal bronchioles (TB-2) were examined with microCT and histology in eight explanted lungs with end-stage COPD and seven unused donor lungs that served as controls.On MDCT, COPD lungs showed a decrease in the number of 2-2.5 mm diameter airways and the lumen area of fifth-generation airways, while on microCT there was a reduction in the number of terminal bronchioles as well as a decrease in the luminal areas, wall volumes and alveolar attachments to the walls of TB, TB-1 and TB-2 bronchioles. The combination of microCT and histology showed increased B-cell infiltration into the walls of TB-1 and TB-2 bronchioles, and this change was correlated with a reduced number of alveolar attachments in COPD.Small airways disease extends from 2 mm diameter airways to the terminal bronchioles in COPD. Destruction of alveolar attachments may be driven by a B-cell-mediated immune response in the preterminal bronchioles.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
Figures
References
-
- Weibel ER. Morphometry of the Human Lung. Springer Verlag and Academic Press, Heidelberg-New York: 1963.
-
- Green M How big are the bronchioles?. St Thomas Hospital gazette 1965: 63: 136–139.
-
- Macklem PT, Mead J. Resistance of central and peripheral airways measured by a retrograde catheter. J Appl Physiol 1967: 22(3): 395–401. - PubMed
-
- Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway obstruction in chronic obstructive lung disease. N Engl J Med 1968: 278(25): 1355–1360. - PubMed
-
- Mead J The lung’s “quiet zone”. N Engl J Med 1970: 282(23): 1318–1319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical