

Increasing Incidence and Prevalence of World Health Organization Groups 1 to 4 Pulmonary Hypertension: A Population-Based Cohort Study in Ontario, Canada
- PMID: 29444925
- PMCID: PMC5819352
- DOI: 10.1161/CIRCOUTCOMES.117.003973
Increasing Incidence and Prevalence of World Health Organization Groups 1 to 4 Pulmonary Hypertension: A Population-Based Cohort Study in Ontario, Canada
Abstract
Background: The World Health Organization recognizes 5 groups of pulmonary hypertension (PH), categorized by pathogenesis or comorbidity: 1-pulmonary arterial hypertension 2-left-heart disease, 3-lung disease and hypoxia 4-chronic thromboembolic disease, and 5-miscellaneous. The epidemiology of PH, apart from group 1, is largely unknown.
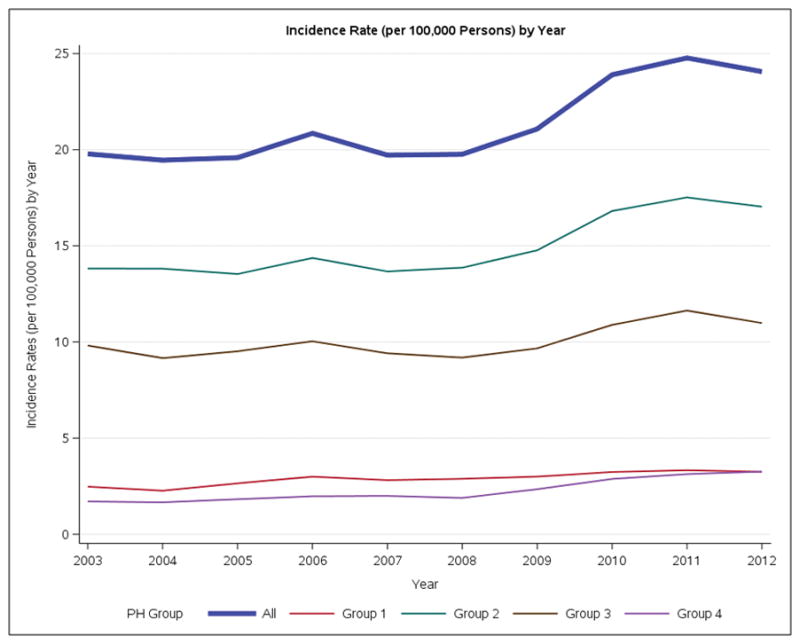
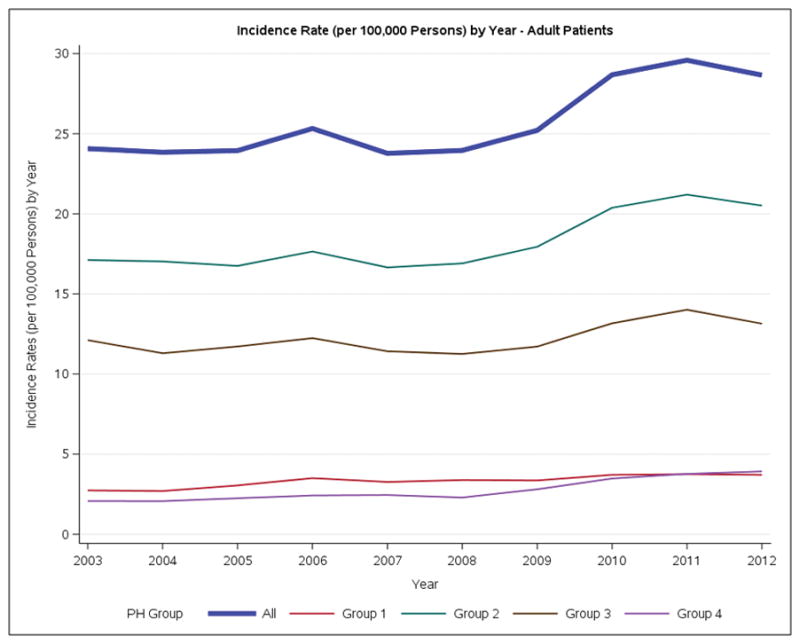
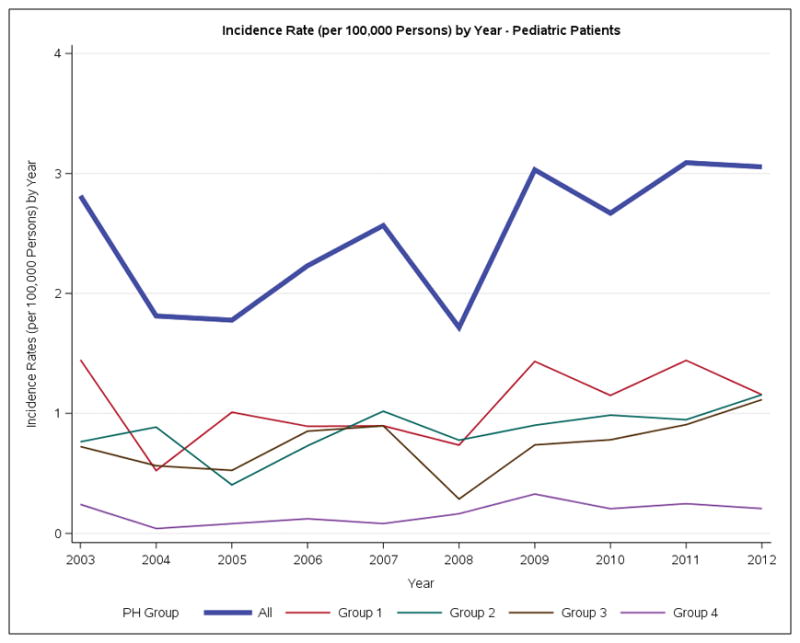
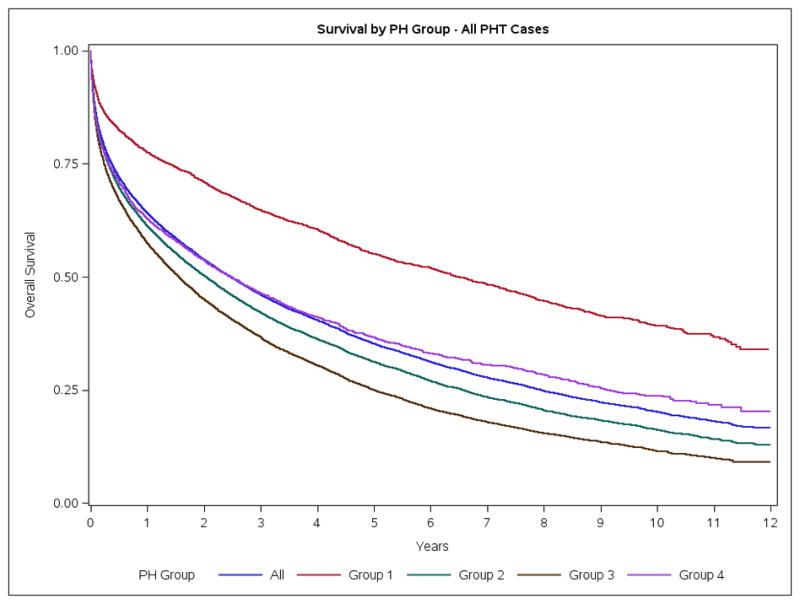
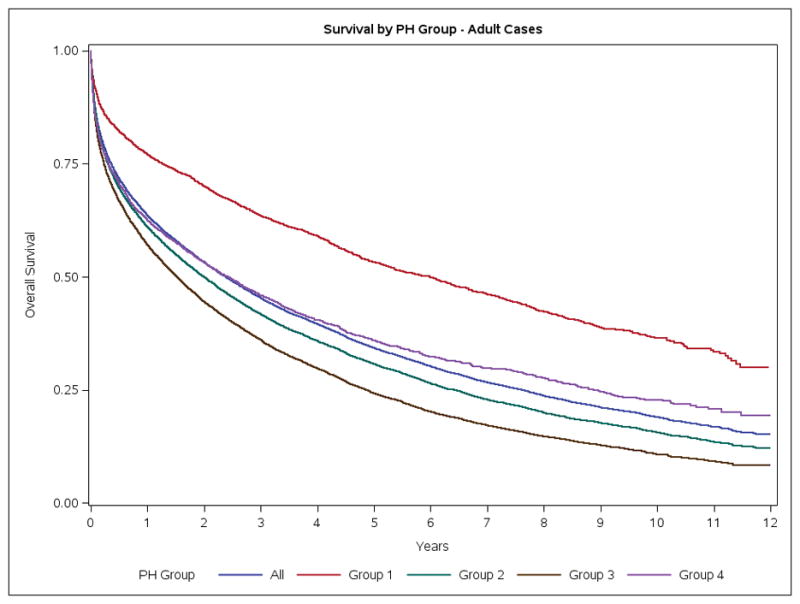
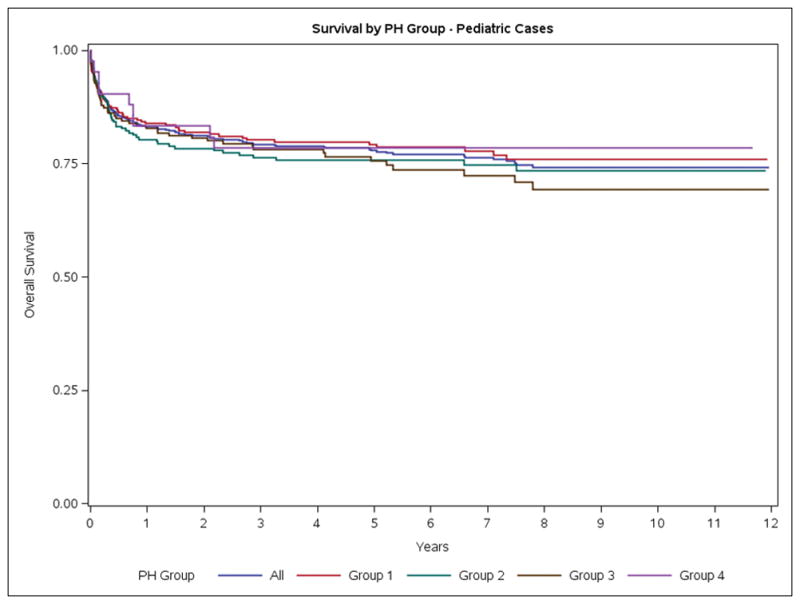
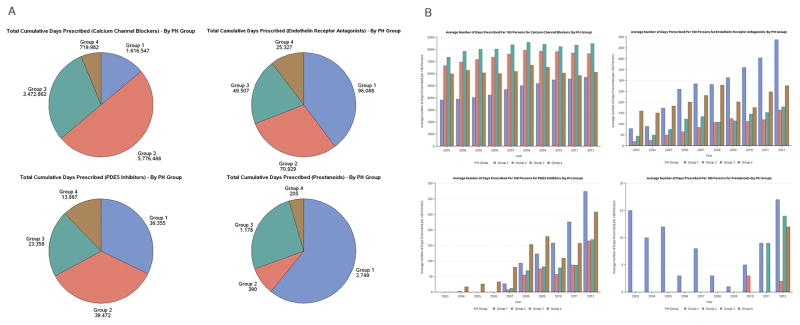
Methods and results: We describe incidence, prevalence, comorbidities, mortality and prescribing patterns for groups 1 to 4 PH from 1993 to 2012. Case definitions are based on hospitalizations and emergency department visits, using the Institute for Clinical Evaluative Sciences data, which comprises linked databases of universal coverage health service records for Ontario residents. This cohort included 50 529 patients with PH. The annual incidence of adult PH increased from 2003 to 2012 from 24.1 to 28.7 cases/100 000 population and the annual prevalence from 1993 to 2012 from 99.8 to 127.3 cases/100 000 population, respectively. The most common form of adult PH was group 2, alone (34.2%) or combined with group 3 PH (29.3%). A diagnosis of PH increased the 1-year standardized mortality ratio 7.2-fold. Mortality in adults with PH was 13.0%, 36.4%, and 62.4%, at 30 days, 1 year, and 5 years, respectively. Mortality was highest in groups 2 and 3 and lowest in group 1. PH was present in only 3.6% of people with left heart disease, 0.7% with lung disease, and 1.4% with thromboembolic disease, suggesting that PH is a relatively rare complication of these common diseases. Children (age<16 years) accounted for 3.6% of the cohort. In children group 1 PH was most common (65.2%), and 5-year mortality was lower (21.4%) than in adults. Group 1-specific PH therapies were increasingly prescribed over time and paradoxically were often used in patients who seemed to have group 2, PH based on diagnostic codes indicating left heart disease.
Conclusions: The incidence and prevalence of adult PH are increasing. Groups 2 and 3 are the most common and lethal forms of PH. This study identifies an emerging epidemic of PH that likely has substantial adverse health and economic implications.
Keywords: comorbidity; heart diseases; hypertension, pulmonary; hypoxia; incidence; lung diseases; prevalence.
© 2018 American Heart Association, Inc.
Figures
Comment in
-
The Growing Burden of Pulmonary Hypertension in the Modern Era: A Zebra No More?Circ Cardiovasc Qual Outcomes. 2018 Feb;11(2):e004536. doi: 10.1161/CIRCOUTCOMES.118.004536. Circ Cardiovasc Qual Outcomes. 2018. PMID: 29444928 No abstract available.
References
-
- Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, Gomez Sanchez MA, Krishna Kumar R, Landzberg M, Machado RF, Olschewski H, Robbins IM, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D34–41. - PubMed
-
- Califf RM, Adams KF, McKenna WJ, Gheorghiade M, Uretsky BF, McNulty SE, Darius H, Schulman K, Zannad F, Handberg-Thurmond E, Harrell FE, Wheeler W, Soler-Soler J, Swedberg K. A randomized controlled trial of epoprostenol therapy for severe congestive heart failure: The Flolan International Randomized Survival Trial (FIRST) American Heart Journal. 1997;134:44–54. - PubMed
-
- Redfield MM, Chen HH, Borlaug BA, Semigran MJ, Lee KL, Lewis G, LeWinter MM, Rouleau JL, Bull DA, Mann DL, Deswal A, Stevenson LW, Givertz MM, Ofili EO, O’Connor CM, Felker GM, Goldsmith SR, Bart BA, McNulty SE, Ibarra JC, Lin G, Oh JK, Patel MR, Kim RJ, Tracy RP, Velazquez EJ, Anstrom KJ, Hernandez AF, Mascette AM, Braunwald E, Trial R. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013;309:1268–77. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
